北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (6): 1159-1164. doi: 10.19723/j.issn.1671-167X.2019.06.032
低功率钬激光“七步两叶法”前列腺剜除术治疗良性前列腺增生
刘可,张帆,肖春雷( ),夏海缀,郝一昌,毕海,赵磊,刘余庆,卢剑,马潞林
),夏海缀,郝一昌,毕海,赵磊,刘余庆,卢剑,马潞林
- 北京大学第三医院泌尿外科,北京 100191
Low power seven-step two-lobe holmium laser enucleation of the prostate technique for surgical treatment of benign prostatic hyperplasia
Ke LIU,Fan ZHANG,Chun-lei XIAO(),Hai-zhui XIA,Yi-chang HAO,Hai BI,Lei ZHAO,Yu-qing LIU,Jian LU,Lu-lin MA
- Department of Urology, Peking University Third Hospital, Beijing 100191, China
摘要:
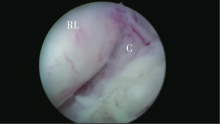
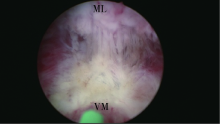
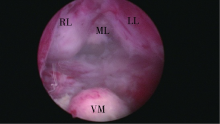
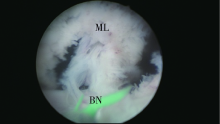
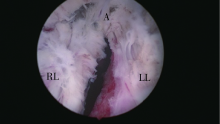
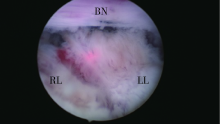
目的 探讨采用低功率钬激光“七步两叶法”行前列腺剜除术的可行性,介绍“七步两叶法”的具体步骤及近期疗效。方法 回顾2016年3月至2017年11月间90例于北京大学第三医院接受经尿道钬激光前列腺剜除术的患者资料,按手术使用钬激光设备不同分为两组,高功率组32例,手术使用高功率钬激光,功率设置为90 W;低功率组58例,手术使用低功率钬激光,功率设置为40 W。手术方法前者采用“三叶法”,即先在5、7点纵行切开腺体至包膜,然后完整剥离中叶,再在12点纵行切开至包膜,先后剥离左右叶,最后离断尖部连接腺体的黏膜,使左右叶腺体完全游离;后者则采用“七步两叶法”,其具体步骤包括:(1)在精阜两侧5、7点找到正确的包膜平面;(2)于精阜近端横行切开使两侧包膜平面相连;(3)向膀胱颈方向扇形剥离腺体与背侧包膜;(4)于尖部5、7点逆行向膀胱颈部分割中叶与左、右叶;(5)完全剥离中叶;(6)于前列腺尖部环行切断尿路黏膜;(7)分别从尖部两侧向腹侧及膀胱颈方向剥离左、右叶并最终于12点汇合使两侧叶完整剥离。结果 高功率组与低功率组患者的平均年龄分别为(66.25±5.37)岁和(68.00±5.18)岁;体重指数平均值分别为(24.13±4.06) kg/m 2和(24.57±3.50) kg/m 2;前列腺特异性抗原平均值分别为(3.23±2.47) μg/L和(6.00±6.09) μg/L;B超测量前列腺体积平均值分别为(49.03±20.63) mL和(67.55±36.97) mL,组间差异均无统计学意义。两组患者的围手术期数据及随访数据,包括手术时间、剜除效率、术后血红蛋白下降程度、术后血钠、血钾变化程度、尿管留置时间、术后住院天数、术前、术后国际前列腺症状评分及生活质量评分等组间差异均无统计学意义。高功率组1例术中中转经尿道前列腺电切术;低功率组1例术中输血。术后1个月随访显示:两组均无明显尿失禁,射精功能障碍高功率组3例,低功率组1例。其他手术相关并发症包括高功率组2例术后活动性出血 (Clavien Ⅱ 及 Clavien Ⅲb);低功率组2例术后发热超过38 ℃ (Clavien Ⅰ), 1例拔尿管后排尿困难 (Clavien Ⅰ)。结论 采用低功率钬激光及“七步两叶法”可安全开展钬激光前列腺剜除术,并取得与高功率钬激光前列腺剜除术相似的疗效。
中图分类号:
- R697 +.3








| [1] | Vincent MW, Gilling PJ . HoLEP has come of age[J]. World J Urol, 2015,33(4):487-493. |
| [2] | Cornu JN, Ahyai S, Bachmann A , et al. A systematic review and meta-analysis of functional outcomes and complications following transurethral procedures for lower urinary tract symptoms resulting from benign prostatic obstruction: an update[J]. Eur Urol, 2015,67(6):1066-1096. |
| [3] | Robert G, Cornu JN, Fourmarier M , et al. Multicentre prospective evaluation of the learning curve of holmium laser enucleation of the prostate (HoLEP)[J]. BJU Int, 2016,117(3):495-499. |
| [4] | 刘宁, 黄广林, 满立波 , 等. 缩短钬激光前列腺剜除术学习曲线的方法[J]. 北京大学学报(医学版), 2015,4(1):720-723. |
| [5] | Becker B, Gross AJ, Netsch C . Safety and efficacy using a low-powered holmium laser for enucleation of the prostate (HoLEP): 12-month results from a prospective low-power HoLEP series[J]. World J Urol, 2018,36(3):441-447. |
| [6] | Gong YG, He DL, Wang MZ , et al. Holmium laser enucleation of the prostate: A modified enucleation technique and initial results[J]. J Urol, 2012,187(4):1336-1340. |
| [7] | Minagawa S, Okada S, Morikawa H . Safety and effectiveness of holmium laser enucleation of the prostate using a low-power laser[J]. Urology, 2017,110:51-55. |
| [8] | Scoffone CM, Cracco CM . High-power HoLEP: No thanks![J]. World J Urol, 2018,36(5):837-838. |
| [9] | 刘可, 肖春雷, 马潞林 . 钬激光前列腺剜除术治疗良性前列腺增生的自学学习曲线[J]. 中国微创外科杂志, 2016,16(1):31-34. |
| [10] | Scoffone CM, Cracco CM . The en-bloc no-touch holmium laser enucleation of the prostate (HoLEP) technique[J]. World J Urol, 2016,34(8):1175-1181. |
| [11] | Kim M, Lee HE, Oh SJ . Technical aspects of holmium laser enucleation of the prostate for benign prostatic hyperplasia[J]. Korean J Urol, 2013,54(9):570-579. |
| [12] | Endo F, Shiga Y, Minagawa S , et al. Anteroposterior dissection HoLEP: A modification to prevent transient stress urinary incontinence[J]. Urology, 2010,76(6):1451-1455. |
| [13] | Elkoushy MA, Elshal AM, Elhiralli MM . Reoperation after hol-mium laser enucleation of the prostate for management of benign prostate hyperplasia: Assessment of risk factors with time to event analysis[J]. J Endourol, 2015,29(7):797-804. |
| [1] | 牛远杰, 辛钟成, 林桂亭, 丁攀, 潘建成, 封玉宏, 郭应禄. 低强度激光疗法治疗男性生殖与性功能障碍[J]. 北京大学学报(医学版), 2025, 57(4): 627-632. |
| [2] | 左超, 王国立, 杨昆霖, 车新艳, 孟一森, 张凯. 前列腺体积不同的患者经尿道光纤铥激光前列腺剜除术的有效性及安全性比较[J]. 北京大学学报(医学版), 2025, 57(4): 711-716. |
| [3] | 柳登高,郑丹妮,赵雅宁,张亚琼,叶欣,张丽琪,谢晓艳,张雷,张祖燕,俞光岩. 疑难唾液腺结石病的治疗研究[J]. 北京大学学报(医学版), 2023, 55(1): 8-12. |
| [4] | 王向熙,李臻臻,赖彦云,杨莉,史霖丽,仲少敏,吴艳. 585 nm Q开关激光治疗痤疮炎症性皮损和炎症后红斑的疗效[J]. 北京大学学报(医学版), 2022, 54(2): 283-288. |
| [5] | 马珂楠,陈虎,沈妍汝,周永胜,王勇,孙玉春. 选择性激光熔化打印可摘局部义齿圆环形卡环固位力的有限元分析[J]. 北京大学学报(医学版), 2022, 54(1): 105-112. |
| [6] | 李文锦,丁茜,原福松,孙丰博,郑剑桥,鲍蕊,张磊. 飞秒激光表面处理对氧化锆表面特征及弯曲强度的影响[J]. 北京大学学报(医学版), 2021, 53(4): 770-775. |
| [7] | 郝一昌,陈昆,刘余庆,卢剑,肖春雷,马潞林. 输尿管软镜下钬激光切除术治疗肾盂癌6例报道及文献复习[J]. 北京大学学报(医学版), 2018, 50(5): 816-821. |
| [8] | 隋华欣,吕培军,王勇,冯驭驰. 低能量激光照射对人脂肪来源干细胞/海藻酸钠/明胶三维生物打印体成骨能力的影响[J]. 北京大学学报(医学版), 2018, 50(5): 868-875. |
| [9] | 修倩,陈曦, 刘潼,陈明星,姚平,辛伟红. 气管切开后再次出现呼吸困难2例及Mimics 10.01软件的临床应用[J]. 北京大学学报(医学版), 2018, 50(5): 924-927. |
| [10] | 刘婧寅,陈飞,葛严军,魏菱,潘韶霞,冯海兰. 选择性激光熔化种植体对早期骨矿化沉积率的影响[J]. 北京大学学报(医学版), 2018, 50(1): 117-122. |
| [11] | 程明轩,姜婷,孙玉春,张皓羽. 比较口内扫描和模型扫描对数字化牙列模型咬合定量分析的影响[J]. 北京大学学报(医学版), 2018, 50(1): 136-140. |
| [12] | 隋华欣, 吕培军, 王宇光, 王勇, 孙玉春. 低能量激光照射对人脂肪基质细胞增殖分化的影响[J]. 北京大学学报(医学版), 2017, 49(2): 337-343. |
| [13] | 苏征,白雨豪,侯晓玫. 不同技术对弯曲根管根尖气锁去除效果的锥形束CT研究[J]. 北京大学学报(医学版), 2017, 49(1): 76-080. |
| [14] | 王莺, Obada Barry, Gerhard Wahl, 陈波,林野. 应用激光多普勒血流仪监测口腔黏膜血流[J]. 北京大学学报(医学版), 2016, 48(4): 697-701. |
| [15] | 郭怡丹,张笋. Er:YAG激光用于比格犬牙髓切断术[J]. 北京大学学报(医学版), 2016, 48(4): 714-719. |
|
||
