北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (5): 850-856. doi: 10.19723/j.issn.1671-167X.2021.05.007
前交叉韧带重建术后膝关节感染的诊断和治疗策略
王成1,孟令宇2,陈拿云1,李玳1,王健全1,敖英芳1,△( )
)
- 1.北京大学第三医院运动医学科,北京大学运动医学研究所,运动医学关节伤病北京市重点实验室,北京 100191
2.北京大学基础医学院,北京 100191
Management algorithm for septic arthritis after anterior cruciate ligament reconstruction
WANG Cheng1,MENG Ling-yu2,CHEN Na-yun1,LI Dai1,WANG Jian-quan1,AO Ying-fang1,△()
- 1. Department of Sports Medicine, Peking University Third Hospital, Institute of Sports Medicine of Peking University, Beijing Key Laboratory of Sports Injuries, Beijing 100191, China
2. Peking University School of Basic Medical Sciences, Beijing 100191, China
摘要:
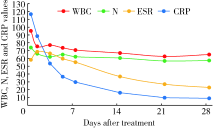
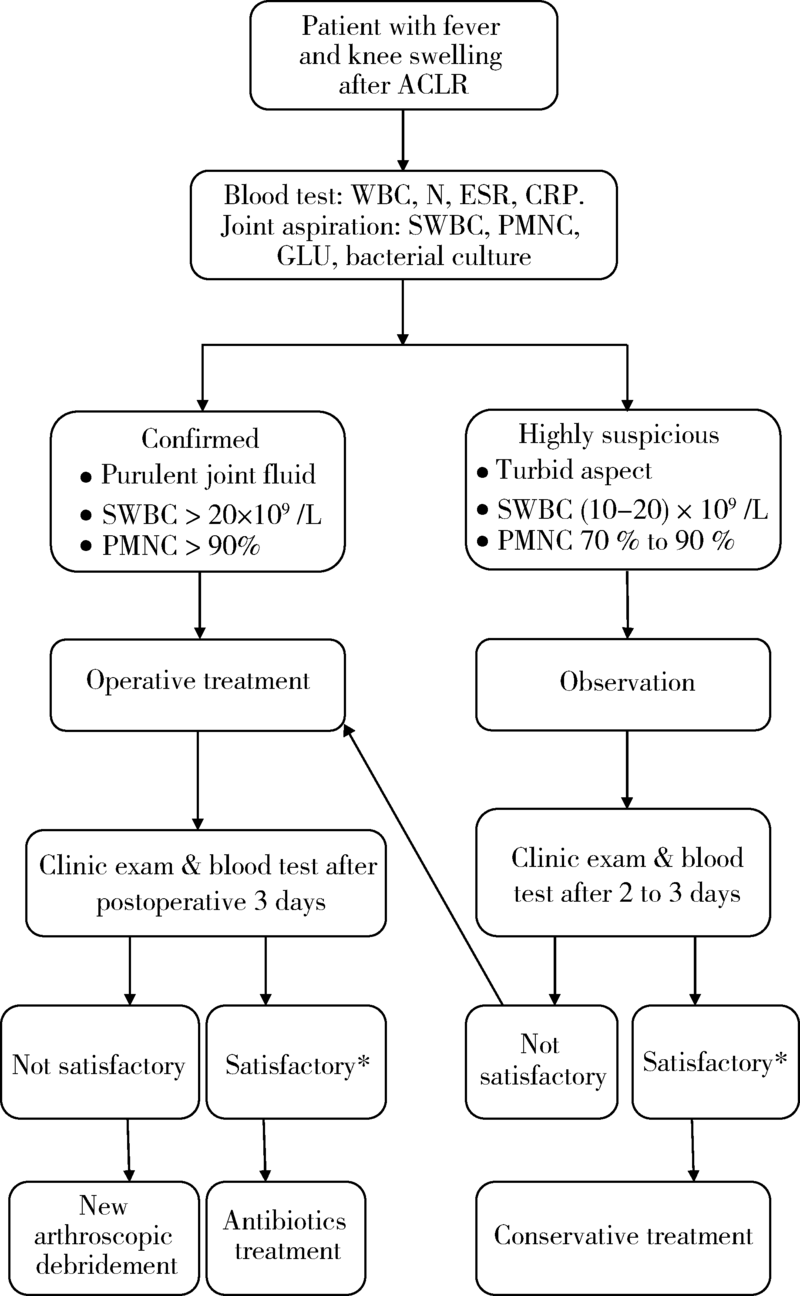
目的: 探讨关节镜下前交叉韧带重建术后膝关节感染的临床诊断和治疗策略。方法: 选择2001年1月至2020年12月在北京大学第三医院运动医学科行关节镜下前交叉韧带重建手术且术后发生膝关节感染的病例进行回顾性分析。通过对患者术后关节感染的发病过程、临床特征、试验室检查、治疗方法及随访结果进行分析,探讨最佳的临床诊断和治疗策略。结果: 20年间关节镜下前交叉韧带重建手术共27 867例,术后膝关节感染65例,感染率0.23%。临床表现有体温增高[(38.7±0.5) ℃]、膝关节肿痛、关节活动度受限。细菌培养阳性率 69.2%,其中凝固酶阴性葡萄球菌(占75.6%)、金黄色葡萄球菌(占15.6%)最常见。保守治疗组(16例)和手术治疗组(49例)均能有效控制感染,但保守治疗组体温恢复较慢(保守治疗组5.6 d,手术治疗组1.6 d,P=0.042)。结论: 前交叉韧带重建术后膝关节感染是一种发生率低,但后果严重的并发症,临床诊断建议及早进行关节腔穿刺和病原学检查,一旦确诊,建议尽早进行关节镜清理手术,并给予有效抗生素治疗。
中图分类号:
- R687


| [1] |
Murawski CD, Wolf MR, Araki D, et al. Anatomic anterior cruciate ligament reconstruction: current concepts and future perspective [J]. Cartilage, 2013, 4(3):27S-37S.
doi: 10.1177/1947603513486557 |
| [2] |
Williams RJ, Laurencin CT, Warren RF, et al. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction. Diagnosis and management [J]. Am J Sports Med, 1997, 25(2):261-267.
doi: 10.1177/036354659702500222 |
| [3] |
McAllister DR, Parker RD, Cooper AE, et al. Outcomes of postoperative septic arthritis after anterior cruciate ligament reconstruction [J]. Am J Sports Med, 1999, 27(5):562-570.
doi: 10.1177/03635465990270050301 |
| [4] |
Viola R, Marzano N, Vianello R. An unusual epidemic of Staphylococcus-negative infections involving anterior cruciate ligament reconstruction with salvage of the graft and function [J]. Arthroscopy, 2000, 16(2):173-177.
pmid: 10705329 |
| [5] |
Indelli PF, Dillingham M, Fanton G, et al. Septic arthritis in postoperative anterior cruciate ligament reconstruction [J]. Clin Orthop Relat Res, 2002, 398:182-188.
doi: 10.1097/00003086-200205000-00026 |
| [6] |
Schollin-Borg M, Michaёlsson K, Rahme H. Presentation, outcome, and cause of septic arthritis after anterior cruciate ligament reconstruction: a case control study [J]. Arthroscopy, 2003, 19(9):941-947.
pmid: 14608312 |
| [7] |
Burks RT, Friederichs MG, Fink B, et al. Treatment of post-operative anterior cruciate ligament infections with graft removal and early reimplantation [J]. Am J Sports Med, 2003, 31(3):414-418.
doi: 10.1177/03635465030310031501 |
| [8] |
Fong SY, Tan JL. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction [J]. Ann Acad Med Singap, 2004, 33(2):228-234.
pmid: 15098639 |
| [9] |
Musso AD, McCormack RG. Infection after ACL reconstruction: what happens when cultures are negative [J]. Clin J Sport Med, 2005, 15(5):381-384.
pmid: 16162999 |
| [10] |
Zalavras CG, Patzakis MJ, Tibone J, et al. Treatment of persistent infection after anterior cruciate ligament surgery [J]. Clin Orthop Relat Res, 2005, 439:52-55.
doi: 10.1097/01.blo.0000181499.49740.e5 |
| [11] |
Judd D, Bottoni C, Kim D, et al. Infections following arthroscopic anterior cruciate ligament reconstruction [J]. Arthroscopy, 2006, 22(4):375-384.
doi: 10.1016/j.arthro.2005.12.002 |
| [12] |
Binnet MS, Basarir K. Risk and outcome of infection after different arthroscopic anterior cruciate ligament reconstruction techniques [J]. Arthroscopy, 2007, 23(8):862-868.
doi: 10.1016/j.arthro.2007.02.008 |
| [13] |
Van Tongel A, Stuyck J, Bellemans J, et al. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction: a retrospective analysis of incidence, management and outcome [J]. Am J Sports Med, 2007, 35(7):1059-1063.
doi: 10.1177/0363546507299443 |
| [14] |
Schulz AP, Götze S, Schmidt HG, et al. Septic arthritis of the knee after anterior cruciate ligament surgery: a stage-adapted treatment regimen [J]. Am J Sports Med, 2007, 35(7):1064-1069.
doi: 10.1177/0363546507299744 |
| [15] |
Katz LM, Battaglia TC, Patino P, et al. A retrospective comparison of the incidence of bacterial infection following anterior cruciate ligament reconstruction with autograft versus allograft [J]. Arthroscopy, 2008, 24(12):1330-1335.
doi: 10.1016/j.arthro.2008.07.015 |
| [16] |
Iorio R, Vadalà A, Di VI, et al. Tunnel enlargement after anterior cruciate ligament reconstruction in patients with post-operative septic arthritis [J]. Knee Surg Sports Traumatol Arthrosc, 2008, 16(10):921-927.
doi: 10.1007/s00167-008-0575-1 |
| [17] |
Wang C, Ao Y, Wang J, et al. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction: a retrospective analysis of incidence, presentation, treatment, and cause [J]. Arthroscopy, 2009, 25(3):243-249.
doi: 10.1016/j.arthro.2008.10.002 |
| [18] | Sajovic M, NiCAGL , Dernovš EMZ. Septic arthritis of the knee following anterior cruciate ligament reconstruction [J]. Orthop Rev (Pavia), 2009, 1(1):e3. |
| [19] |
Nag HL, Neogi DS, Nataraj AR, et al. Tubercular infection after arthroscopic anterior cruciate ligament reconstruction [J]. Arthroscopy, 2009, 25(2):131-136.
doi: 10.1016/j.arthro.2008.09.009 |
| [20] |
Monaco E, Maestri B, Labianca L, et al. Clinical and radiological outcomes of postoperative septic arthritis after anterior cruciate ligament reconstruction [J]. J Orthop Sci, 2010, 15(2):198-203.
doi: 10.1007/s00776-009-1447-3 |
| [21] |
Barker JU, Drakos MC, Maak TG, et al. Effect of graft selection on the incidence of postoperative infection in anterior cruciate ligament reconstruction [J]. Am J Sports Med, 2010, 38(2):281-286.
doi: 10.1177/0363546509346414 |
| [22] |
Benner RW, Shelbourne KD, Freeman H. Infections and patellar tendon ruptures after anterior cruciate ligament reconstruction: a comparison of ipsilateral and contralateral patellar tendon autografts [J]. Am J Sports Med, 2011, 39(3):519-525.
doi: 10.1177/0363546510388163 |
| [23] |
Sonnery-Cottet B, Archbold P, Zayni R, et al. Prevalence of septic arthritis after anterior cruciate ligament reconstruction among professional athletes [J]. Am J Sports Med, 2011, 39(11):2371-2376.
doi: 10.1177/0363546511417567 pmid: 21856928 |
| [24] |
Vertullo CJ, Quick M, Jones A, et al. A surgical technique using presoaked vancomycin hamstring grafts to decrease the risk of infection after anterior cruciate ligament reconstruction [J]. Arthroscopy, 2012, 28(3):337-342.
doi: 10.1016/j.arthro.2011.08.301 |
| [25] |
Schub DL, Schmitz LM, Sakamoto FA, et al. Long-term outcomes of postoperative septic arthritis after anterior cruciate ligament reconstruction [J]. Am J Sports Med, 2012, 40(12):2764-2770.
doi: 10.1177/0363546512461903 |
| [26] |
Torres-Claramunt R, Pelfort X, Erquicia J, et al. Knee joint infection after ACL reconstruction: prevalence, management and functional outcomes [J]. Knee Surg Sports Traumatol Arthrosc, 2013, 21(12):2844-2849.
doi: 10.1007/s00167-012-2264-3 |
| [27] |
RisticV , Maljanovic M, Harhaji V, et al. Infections after reconstructions of anterior cruciate ligament [J]. Med Pregl, 2014, 67(1/2):11-15.
doi: 10.2298/MPNS1402011R |
| [28] |
Abdel-Aziz A, Radwan YA, Rizk A. Multiple arthroscopic debridement and graft retention in septic knee arthritis after ACL reconstruction: a prospective case-control study [J]. Int Orthop, 2014, 38(1):73-82.
doi: 10.1007/s00264-013-2123-y pmid: 24100920 |
| [29] |
Boström WH, Mikkelsen C, Forssblad M, et al. Postoperative septic arthritis after anterior cruciate ligament reconstruction: does it affect the outcome? a retrospective controlled study [J]. Arthroscopy, 2014, 30(9):1100-1109.
doi: 10.1016/j.arthro.2014.03.019 |
| [30] |
Calvo R, Figueroa D, Anastasiadis Z, et al. Septic arthritis in ACL reconstruction surgery with hamstring autografts. eleven years of experience [J]. Knee, 2014, 21(3):717-720.
doi: 10.1016/j.knee.2014.01.007 |
| [31] |
Schuster P, Schulz M, Immendoerfer M, et al. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction: evaluation of an arthroscopic graft-retaining treatment protocol [J]. Am J Sports Med, 2015, 43(12):3005-3012.
doi: 10.1177/0363546515603054 pmid: 26403209 |
| [32] |
Pérez-Prieto D, Trampuz A, Torres-Claramunt R, et al. Infections after anterior cruciate ligament reconstruction: which antibiotic after arthroscopic debridement? [J]. J Knee Surg, 2017, 30(4):309-313.
doi: 10.1055/s-0036-1584559 pmid: 27367205 |
| [33] |
Hantes ME, Raoulis VA, Doxariotis N, et al. Management of septic arthritis after arthroscopic anterior cruciate ligament reconstruction using a standard surgical protocol [J]. Knee, 2017, 24(3):588-593.
doi: 10.1016/j.knee.2017.02.007 |
| [34] |
Torres-Claramunt R, Gelber P, Pelfort X, et al. Managing septic arthritis after knee ligament reconstruction [J]. Int Orthop, 2016, 40(3):607-614.
doi: 10.1007/s00264-015-2884-6 pmid: 26239533 |
| [35] |
Wang C, Lee YH, Siebold R. Recommendations for the management of septic arthritis after ACL reconstruction [J]. Knee Surg Sports Traumatol Arthrosc, 2014, 22(9):2136-2144.
doi: 10.1007/s00167-013-2648-z |
| [36] |
Muscolo DL, Carbo L, Aponte-Tinao LA, et al. Massive bone loss from fungal infection after anterior cruciate ligament arthroscopic reconstruction [J]. Clin Orthop Relat Res, 2009, 467(9):2420-2425.
doi: 10.1007/s11999-009-0714-0 |
| [37] |
Wang C, Ao Y, Fan X, et al. C-reactive protein and erythrocyte sedimentation rate changes after arthroscopic anterior cruciate ligament reconstruction: guideline to diagnose and monitor postoperative infection [J]. Arthroscopy, 2014, 30(9):1110-1115.
doi: 10.1016/j.arthro.2014.03.025 |
| [38] |
Paci JM, Schweizer SK, Wilbur DM, et al. Results of laboratory evaluation of acute knee effusion after anterior cruciate ligament reconstruction: what is found in patients with a noninfected, painful postoperative knee [J]. Am J Sports Med, 2010, 38(11):2267-2272.
doi: 10.1177/0363546510374573 |
| [1] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [2] | 田雪丽, 宋志强, 黄永辉, 姚炜. 肌萎缩侧索硬化患者经皮内镜下胃造瘘术后早期并发症及相关危险因素分析[J]. 北京大学学报(医学版), 2026, 58(1): 190-195. |
| [3] | 王晓林, 郭邵逸, 陈大召, 温锡杰, 华勇, 张亮, 张秦. 全髋关节置换术治疗系统性红斑狼疮继发股骨头缺血性坏死的随访研究[J]. 北京大学学报(医学版), 2025, 57(6): 1081-1088. |
| [4] | 胡枫艺, 孟庆阳, 陈拿云, 王佳宁, 刘振龙, 马勇, 杨渝平, 龚熹, 王成, 刘平, 史尉利. 镜下内侧髌股复合体重建治疗伴高级别滑车发育不良复发性髌骨脱位的临床疗效[J]. 北京大学学报(医学版), 2025, 57(5): 947-955. |
| [5] | 余霄腾, 黄奕瑄, 李新飞, 陈昶甫, 赵方舟, 应鸿刚, 陶子豪, 张一鸣, 徐丽清, 李志华, 杨昆霖, 周利群, 李学松, 赵峥. 结石相关输尿管狭窄的上尿路修复手术技术与临床结局[J]. 北京大学学报(医学版), 2025, 57(4): 670-675. |
| [6] | 左超, 王国立, 杨昆霖, 车新艳, 孟一森, 张凯. 前列腺体积不同的患者经尿道光纤铥激光前列腺剜除术的有效性及安全性比较[J]. 北京大学学报(医学版), 2025, 57(4): 711-716. |
| [7] | 赵兆, 张维宇, 杨文博, 张勇杰, 张晓鹏, 赵慧颖, 周刚, 王强. 低龄、低体重儿童肾移植2例[J]. 北京大学学报(医学版), 2025, 57(4): 803-807. |
| [8] | 孙建军, 马千权, 尹晓亮, 杨辰龙, 张嘉, 陈素华, 吴超, 谢京城, 韩芸峰, 林国中, 司雨, 杨军, 邬海博, 赵强. 任意维度重建磁共振对骶管囊肿进行精准分型对于指导微创手术和康复的意义[J]. 北京大学学报(医学版), 2025, 57(2): 303-308. |
| [9] | 仇师禹, 练洋, 康一帆, 张雷, 蔡义望, 单小峰, 蔡志刚. 基于下颌骨数据库和全连接神经网络的三维检索模型辅助下的下颌骨个性化重建[J]. 北京大学学报(医学版), 2025, 57(2): 360-368. |
| [10] | 王菲, 张馨月, 刘木清, 王恩博, 段登辉. 顺牙长轴拔牙法在下颌近中与水平智齿拔除术中的应用及三维有限元分析[J]. 北京大学学报(医学版), 2025, 57(1): 106-112. |
| [11] | 马建勋, 布希, 李比. 双腔圆形软组织扩张器在即刻乳房重建中的应用[J]. 北京大学学报(医学版), 2025, 57(1): 166-171. |
| [12] | 王丽薇, 刘冰川, 曲音音, 吴长毅, 田耘. 多学科诊疗模式在慢性难愈合创面诊疗中的临床应用[J]. 北京大学学报(医学版), 2025, 57(1): 185-191. |
| [13] | 谢芳菲, 乔虹, 李博雅, 袁翠, 王芳, 孙瑜, 李双玲. 妊娠期重度营养不良合并急性肾盂肾炎致脓毒症、难治性感染性休克、多器官功能衰竭1例[J]. 北京大学学报(医学版), 2025, 57(1): 202-207. |
| [14] | 聂骏男, 董佳芸, 路瑞芳. 骨瓣重建颌骨区域角化黏膜增量术后软组织愈合效果分析[J]. 北京大学学报(医学版), 2025, 57(1): 57-64. |
| [15] | 康一帆, 葛严军, 吕晓鸣, 谢尚, 单小峰, 蔡志刚. 即刻种植体支持式义齿修复的血管化髂骨瓣重建下颌骨缺损[J]. 北京大学学报(医学版), 2025, 57(1): 78-84. |
|
||
