北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (2): 335-339. doi: 10.19723/j.issn.1671-167X.2022.02.022
腮腺微小肿瘤的临床病理研究
李炳雨,唐祖南,胡耒豪,章文博,于尧,俞光岩,彭歆( )
)
- 北京大学口腔医学院·口腔医院口腔颌面外科,国家口腔医学中心,国家口腔疾病临床医学研究中心,口腔生物材料和数字诊疗装备国家工程研究中心,口腔数字医学北京市重点实验室,北京 100081
Clinicopathologic analysis of micro and mini parotid gland tumors
LI Bing-yu,TANG Zu-nan,HU Lei-hao,ZHANG Wen-bo,YU Yao,YU Guang-yan,PENG Xin()
- Department of Oral and Maxillofacial Surgery, Peking University School and Hospital of Stomatology & National Center of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Research Center of Oral Biomaterials and Digital Medical Devices & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
摘要:
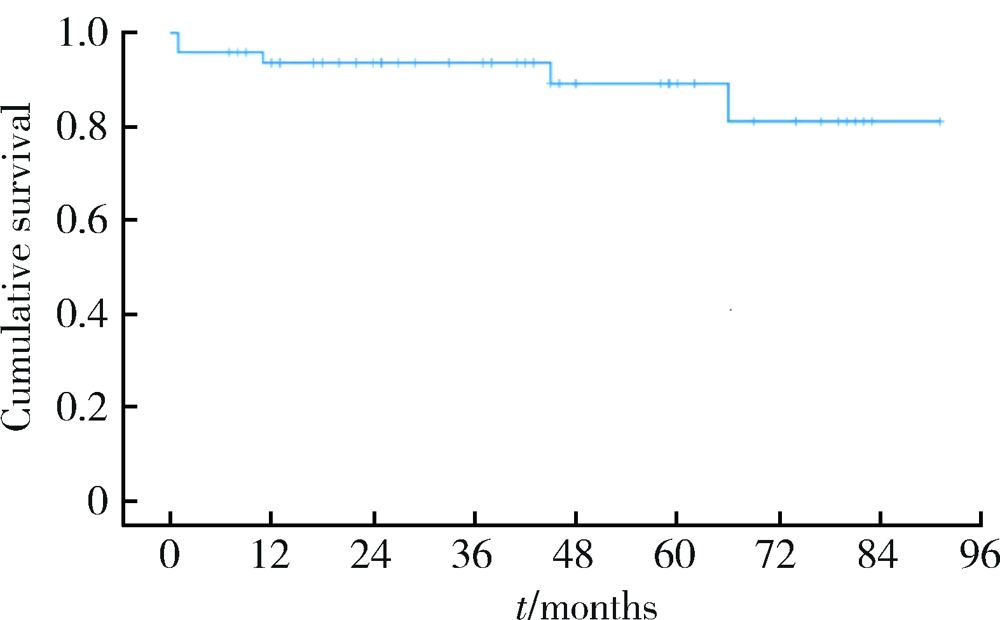
目的: 探讨直径≤20 mm的体积微小的腮腺肿瘤临床病理特点,为临床诊疗提供参考依据。方法: 选择2012年12月至2020年4月于北京大学口腔医院口腔颌面外科手术治疗的腮腺肿瘤患者,收集术前CT检查肿瘤直径≤20 mm的患者相关临床资料,根据肿瘤直径大小分为直径11~20 mm组与直径≤10 mm组,对两组进行临床随访,比较一般情况、临床病理特点及预后。结果: 共收集原发性上皮性腮腺肿瘤患者2 067例,其中肿瘤直径≤20 mm者有685例(33.1%),男女性别比例为1 ∶1.93,平均年龄(45.3±13.8)岁(12~83岁),中位病程12个月(1周至30年)。685例中良性肿瘤635例(92.7%), 恶性肿瘤50例(7.3%),良恶性比例为12.7 ∶1;最常见的良性肿瘤为多形性腺瘤,最常见的恶性肿瘤为黏液表皮样癌。肿瘤直径≤10 mm的患者有74例,占肿瘤直径≤20 mm患者的10.8%(74/685)。肿瘤直径11~20 mm组(n=611)和≤10 mm组(n=74)患者的一般情况及病理学分型比较提示,两组在性别、年龄、病程上差异均无统计学意义(P>0.05)。直径11~20 mm组患者良性肿瘤占92.8%(567/611), 恶性肿瘤占7.2%(44/611), 良恶性比例为12.9 ∶1;直径≤10 mm组良性肿瘤占91.9%(68/74), 恶性肿瘤占8.1%(6/74),良恶性比例为11.3 ∶1,两者间差异无统计学意义(P>0.05)。对50例恶性肿瘤患者进行临床随访,中位随访时间为39.5个月(1~91个月),有2例患者局部复发,其中1例死亡,总体2年生存率为93.7%, 5年生存率为89.3%。结论: 直径≤20 mm的体积微小的腮腺肿瘤以良性多见,手术是主要治疗手段,其中的腮腺恶性肿瘤预后良好,应积极进行早期手术治疗。
中图分类号:
- R739.87

| [1] | 俞光岩, 高岩, 孙永刚, 等. 口腔颌面部肿瘤[M]. 北京: 人民卫生出版社, 2002: 324-381. |
| [2] | 陈志奎, 张秀娟, 黄静, 等. 高频超声诊断腮腺肿瘤[J]. 中国医学影像技术, 2011, 27(9):1775-1778. |
| [3] | 张翔云, 保继荣. 腮腺区肿块影像学综合诊断的临床研究[J]. 广西医科大学学报, 2000, 17(2):231-232. |
| [4] |
Altin F, Alimoglu Y, Acikalin RM, et al. Is fine needle aspiration biopsy reliable in the diagnosis of parotid tumors? Comparison of preoperative and postoperative results and the factors affecting accuracy[J]. Braz J Otorhinolaryngol, 2019, 85(3):275-281.
doi: 10.1016/j.bjorl.2018.04.015 |
| [5] | 中国抗癌协会甲状腺癌专业委员会(CATO). 甲状腺微小乳头状癌诊断与治疗中国专家共识(2016版)[J]. 中国肿瘤临床, 2016, 43(10):405-411. |
| [6] | 付鹏, 陈文, 崔立刚, 等. 2017版美国放射学会甲状腺影像学报告与数据系统应用价值探索[J]. 北京大学学报(医学版), 2019, 51(6):1067-1070. |
| [7] | El-Naggar AK, Chan JK, Grandis JR, et al. WHO classification of tumors of head and neck tumours[M]. 4th ed. Lyon: IARC Press, 2017: 159-201. |
| [8] |
Wong DS. Signs and symptoms of malignant parotid tumours: An objective assessment[J]. J R Coll Surg Edinb, 2001, 46(2):91-95.
pmid: 11329749 |
| [9] |
Cho HW, Kim J, Choi J, et al. Sonographically guided fine-needle aspiration biopsy of major salivary gland masses: A review of 245 cases[J]. Am J Roentgenol, 2011, 196(5):1160-1163.
doi: 10.2214/AJR.10.4256 |
| [10] | Rosai J. ROSAI & ACKERMAN外科病理学[M]. 北京: 北京大学医学出版社, 2014. |
| [11] | Qin S. Guidelines on the diagnosis and treatment of primary liver cancer (2011 edition)[J]. Chin Clin Oncol, 2012, 1(1):10. |
| [12] | 宋勇, 姚艳雯. 肺部小结节的诊断和治疗近况[J]. 中华肺部疾病杂志: 电子版, 2012, 5(4):295-299. |
| [13] |
Macmahon H. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society[J]. Radiology, 2005, 237(2):395-400.
doi: 10.1148/radiol.2372041887 |
| [14] | 王俊, 刘彦国. 肺内小结节的诊治现状、问题和方向[J]. 中华胸心血管外科杂志, 2012, 28(7):385-386. |
| [15] | 凌云, 张明琼, 李芳, 等. 高频彩超、钼靶联合MRI对降低乳腺微小癌漏诊误诊率的价值分析[J]. 检验医学与临床, 2016, 13(21):3004-3005. |
| [16] | 薛杰, 曹小丽, 姜宏, 等. 甲状腺影像报告与数据系统联合超声弹性成像对甲状腺良恶性结节的诊断价值[J]. 中国医学影像学杂志, 2015, 23(5):351-355. |
| [17] |
Rago T, Santini F, Scutari M, et al. Elastography: New developments in ultrasound for predicting malignancy in thyroid nodules[J]. J Clin Endocrinol Metab, 2007, 92(8):2917-2922.
doi: 10.1210/jc.2007-0641 |
| [18] | 陈少卿, 刘钰, 黎军和, 等. 103例腮腺癌的治疗疗效和预后因素分析[J]. 中国肿瘤临床, 2014, 41(12):797-800. |
| [19] | 皮正超, 李长青. 腮腺恶性肿瘤的术后放疗[J]. 中华放射肿瘤学杂志, 1995, 4(3):173-174. |
| [20] | 温玉明, 陈润良, 王昌美. 腮腺多形性腺瘤腺体切除范围的病理依据[J]. 华西口腔医学杂志, 2003, 21(5):359-360. |
| [21] | 俞光岩, 马大权. 腮腺肿瘤切除术的改进和发展[J]. 中华口腔医学杂志, 2007, 42(1):6-9. |
| [22] | 高敏, 陈艳, 高岩, 等. 紧贴面神经的腮腺多形性腺瘤的临床病理特点及处理[J]. 北京大学学报(医学版), 2012, 44(1):43-46. |
| [1] | 王晓林, 李璐瑶, 张雯, 王鸿雁. 3例子宫体中肾样腺癌的临床病理学分析[J]. 北京大学学报(医学版), 2025, 57(6): 1208-1212. |
| [2] | 王小梦, 曾晓君, 李娟. 黎族与汉族系统性红斑狼疮患者的主要临床特征[J]. 北京大学学报(医学版), 2025, 57(6): 1213-1218. |
| [3] | 孙建军, 马千权, 尹晓亮, 杨辰龙, 张嘉, 陈素华, 吴超, 谢京城, 韩芸峰, 林国中, 司雨, 杨军, 邬海博, 赵强. 任意维度重建磁共振对骶管囊肿进行精准分型对于指导微创手术和康复的意义[J]. 北京大学学报(医学版), 2025, 57(2): 303-308. |
| [4] | 王红彦, 李鑫铭, 房柯池, 朱华群, 贾汝琳, 王晶. 系统性红斑狼疮疾病活动度相关特征分析及评估模型的构建[J]. 北京大学学报(医学版), 2024, 56(6): 1017-1022. |
| [5] | 罗丹, 黄海建, 陈新, 陈小岩. 原发子宫肝样腺癌2例临床病理分析及文献复习[J]. 北京大学学报(医学版), 2024, 56(6): 1126-1131. |
| [6] | 赵亮, 史成龙, 马柯, 赵静, 王潇, 邢晓燕, 莫万星, 练益瑞, 高超, 李玉慧. 抗合成酶综合征重叠类风湿关节炎患者的免疫学特征[J]. 北京大学学报(医学版), 2024, 56(6): 972-979. |
| [7] | 邢念增,王明帅,杨飞亚,尹路,韩苏军. 前列腺免活检创新理念的临床实践及其应用前景[J]. 北京大学学报(医学版), 2024, 56(4): 565-566. |
| [8] | 田宇轩,阮明健,刘毅,李德润,吴静云,沈棋,范宇,金杰. 双参数MRI改良PI-RADS评分4分和5分病灶的最大径对临床有意义前列腺癌的预测效果[J]. 北京大学学报(医学版), 2024, 56(4): 567-574. |
| [9] | 刘帅,刘磊,刘茁,张帆,马潞林,田晓军,侯小飞,王国良,赵磊,张树栋. 伴静脉癌栓的肾上腺皮质癌的临床治疗及预后[J]. 北京大学学报(医学版), 2024, 56(4): 624-630. |
| [10] | 赖展鸿,李嘉辰,贠泽霖,张永刚,张昊,邢晓燕,邵苗,金月波,王乃迪,李依敏,李玉慧,栗占国. 特发性炎性肌病完全临床应答相关因素的单中心真实世界研究[J]. 北京大学学报(医学版), 2024, 56(2): 284-292. |
| [11] | 徐训敏,邵校,姬爱平. 口腔急诊科死亡病例分析[J]. 北京大学学报(医学版), 2024, 56(1): 185-189. |
| [12] | 冯璐,翟佳羽,赵金霞. IgG4相关性疾病患者就诊情况及其临床特征[J]. 北京大学学报(医学版), 2023, 55(6): 1028-1032. |
| [13] | 薛子璇,唐世英,邱敏,刘承,田晓军,陆敏,董靖晗,马潞林,张树栋. 青年肾肿瘤伴瘤栓的临床病理特征及预后分析[J]. 北京大学学报(医学版), 2023, 55(5): 802-811. |
| [14] | 魏慧,次旦央宗,益西拉姆,白玛央金. 高原地区不同类型过敏性紫癜藏族患者发病的相关危险因素[J]. 北京大学学报(医学版), 2023, 55(5): 923-928. |
| [15] | 时云飞,王豪杰,刘卫平,米岚,龙孟平,刘雁飞,赖玉梅,周立新,刁新婷,李向红. 血管免疫母细胞性T细胞淋巴瘤临床与分子病理学特征分析[J]. 北京大学学报(医学版), 2023, 55(3): 521-529. |
|
||
