北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (5): 954-960. doi: 10.19723/j.issn.1671-167X.2022.05.024
儿童直立不耐受和坐位不耐受的疾病谱及治疗方式十年回顾
崔雅茜1,杜军保1,2,张清友1,廖莹1,刘平1,王瑜丽1,齐建光1,闫辉1,徐文瑞1,刘雪芹1,孙燕1,孙楚凡1,张春雨1,陈永红1,金红芳1,*( )
)
- 1. 北京大学第一医院儿科, 北京 100034
2. 教育部分子心血管学重点实验室, 北京 100191
A 10-year retrospective analysis of spectrums and treatment options of orthostatic intolerance and sitting intolerance in children
Ya-xi CUI1,Jun-bao DU1,2,Qing-you ZHANG1,Ying LIAO1,Ping LIU1,Yu-li WANG1,Jian-guang QI1,Hui YAN1,Wen-rui XU1,Xue-qin LIU1,Yan SUN1,Chu-fan SUN1,Chun-yu ZHANG1,Yong-hong CHEN1,Hong-fang JIN1,*()
- 1. Department of Pediatrics, Peking University First Hospital, Beijing 100034, China
2. Key Laboratory of Molecular Cardiovascular Sciences, Ministry of Education, Beijing 100191, China
摘要:
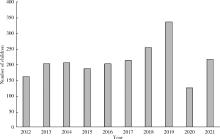
目的: 分析儿童直立不耐受(orthostatic intolerance, OI)和坐位不耐受(sitting intolerance, SI)的基础疾病谱, 并了解其在临床上采用的经验性治疗方式。方法: 选择北京大学第一医院儿科2012年1月至2021年12月十年期间所有患儿的病例资料(包括病史、体格检查、实验室检查和影像学检查)进行回顾性分析, 将符合OI和SI诊断标准的患儿纳入研究, 分析患儿OI和SI的基础疾病谱, 并总结分析其治疗方式。结果: 共纳入OI和SI病例资料2 110例, 其中男943例(44.69%), 女1 167例(55.31%), 年龄4~18岁, 平均(11.34±2.84)岁。十年间总体OI和SI患儿例数呈逐渐增多趋势。OI疾病谱中占比最高的是体位性心动过速综合征(postural orthostatic tachycardia syndrome, POTS), 共826例(39.15%); 其次为血管迷走性晕厥(vasovagal syncope, VVS), 共634例(30.05%)。而SI疾病谱中占比最高的是坐位性心动过速综合征(sitting tachycardia syndrome, STS), 共8例(0.38%); 其次为坐位性高血压(sitting hypertension, SHT) 2例(0.09%); 此外, OI和SI合并疾病中占比最多的是POTS合并STS, 共36例(1.71%)。在OI和SI治疗方式中, 主要为自主神经功能锻炼757例(35.88%), 其次为口服补液盐(oral rehydration salts, ORS) 687例(32.56%), 美托洛尔307例(14.55%), 盐酸米多君142例(6.73%), ORS联合美托洛尔138例(6.54%)和ORS联合盐酸米多君79例(3.74%)。POTS合并VVS的患儿相对于POTS或VVS患儿, 接受药物治疗者更多(41.95% vs. 30.51% vs. 28.08%, χ2= 20.319, P < 0.01), 而POTS和VVS患儿的药物治疗占比没有统计学差异。结论: 儿童POTS及VVS是OI的主要基础疾病, SI是近年来新发现的疾病。OI和SI患儿的人数整体呈逐渐增加的趋势, 其主要治疗方式为自主神经功能锻炼和口服ORS。POTS合并VVS的患儿相对于单纯POTS或VVS患儿, 更倾向于接受药物治疗。
中图分类号:
- R725

| 1 |
魏红芳, 董湘玉, 肖要. 儿童直立不耐受与微观营养素和体质指数相关性研究进展[J]. 中国循证儿科杂志, 2019, 14 (6): 473.
doi: 10.3969/j.issn.1673-5501.2019.06.017 |
| 2 |
Anderson JB , Willis M , Lancaster H , et al. The evaluation and management of pediatric syncope[J]. Pediatr Neurol, 2016, 55, 6- 13.
doi: 10.1016/j.pediatrneurol.2015.10.018 |
| 3 | Jug J , Lovrić Benčić M , Bradić L , et al. Depression, anxiety and quality of life in patients with syncope[J]. Psychiatr Danub, 2020, 32 (3/4): 442- 443. |
| 4 |
Kara A , Doǧan MT . The psychopathology, depression, and anxiety levels of children and adolescents with vasovagal syncope: A case-control study[J]. J Nerv Ment Dis, 2021, 209 (8): 547- 551.
doi: 10.1097/NMD.0000000000001334 |
| 5 |
Zhao J , Han Z , Zhang X , et al. A cross-sectional study on upright heart rate and BP changing characteristics: Basic data for estab-lishing diagnosis of postural orthostatic tachycardia syndrome and orthostatic hypertension[J]. BMJ open, 2015, 5 (6): e007356.
doi: 10.1136/bmjopen-2014-007356 |
| 6 |
Lin J , Wang Y , Ochs T , et al. Tilt angles and positive response of head-up tilt test in children with orthostatic intolerance[J]. Cardiol Young, 2015, 25 (1): 76- 80.
doi: 10.1017/S1047951113001601 |
| 7 | 尚丽丽, 彭宇阁, 刘佳, 等. 直立倾斜试验在儿童不明原因晕厥诊断中的应用[J]. 中国实用神经疾病杂志, 2019, 22 (18): 2026- 2031. |
| 8 |
王利平, 杜忠东, 柴晓敏, 等. 舌下含服硝酸甘油直立倾斜试验对儿童血管迷走性晕厥的诊断价值[J]. 临床儿科杂志, 2006, 24 (5): 364- 366.
doi: 10.3969/j.issn.1000-3606.2006.05.007 |
| 9 |
张清友, 杜军保, 李万镇. 舌下含化硝酸甘油直立倾斜试验对儿童不明原因晕厥的诊断研究[J]. 中华儿科杂志, 2004, 42 (5): 371- 374.
doi: 10.3760/j.issn:0578-1310.2004.05.016 |
| 10 |
Tao C , Han Z , Yan Y , et al. Sitting-induced hemodynamic changes and association with sitting intolerance in children and adolescents: A cross-sectional study[J]. Sci Rep, 2020, 10 (1): 13921.
doi: 10.1038/s41598-020-70925-y |
| 11 |
Wang C , Li Y , Liao Y , et al. 2018 Chinese pediatric cardiology society (CPCS) guideline for diagnosis and treatment of syncope in children and adolescents[J]. Sci Bull, 2018, 63 (23): 1558- 1564.
doi: 10.1016/j.scib.2018.09.019 |
| 12 |
宋婧媛, 王圆圆, 李红霞, 等. 儿童血管迷走性晕厥发病机制研究进展[J]. 中华实用儿科临床杂志, 2018, 33 (6): 478- 480.
doi: 10.3760/cma.j.issn.2095-428X.2018.06.020 |
| 13 |
Magkas N , Tsioufis C , Thomopoulos C , et al. Orthostatic hypotension: From pathophysiology to clinical applications and therapeutic considerations[J]. J Clin Hypertens (Greenwich), 2019, 21 (5): 546- 554.
doi: 10.1111/jch.13521 |
| 14 |
Zhang Q , Li J , Xie Y , et al. Orthostatic hypertension in children and adolescents with postural tachycardia syndrome[J]. J Trop Pediatr, 2014, 60 (6): 461- 466.
doi: 10.1093/tropej/fmu055 |
| 15 |
Brignole M , Moya A , de Lange FJ , et al. 2018 ESC guidelines for the diagnosis and management of syncope[J]. Eur Heart J, 2018, 39 (21): 1883- 1948.
doi: 10.1093/eurheartj/ehy037 |
| 16 | 蔺婧, 王瑜丽, 张清友, 等. 儿童青少年晕厥疾病谱近30年变化及卫生经济学分析单中心报告[J]. 中国实用儿科杂志, 2016, 31 (5): 350- 355. |
| 17 |
杜军保, 李万镇. 基础直立倾斜试验对儿童不明原因晕厥的诊断研究[J]. 中华儿科杂志, 1997, 35 (6): 309- 312.
doi: 10.3760/j.issn:0578-1310.1997.06.008 |
| 18 |
张清友, 杜军保, 李万镇. 儿童体位性心动过速综合征的临床特征及随访研究[J]. 中华儿科杂志, 2005, 43 (3): 165- 169.
doi: 10.3760/j.issn:0578-1310.2005.03.002 |
| 19 | 钟睛. 儿童直立不耐受559例临床分析[D]. 济南: 山东大学, 2019. |
| 20 |
Cai H , Wang S , Zou R , et al. Comparison of the active sitting test and head-up tilt test for diagnosis of postural tachycardia syndrome in children and adolescents[J]. Front Pediatr, 2021, 9, 691390.
doi: 10.3389/fped.2021.691390 |
| 21 |
Kanjwal K , Sheikh M , Karabin B , et al. Neurocardiogenic syncope coexisting with postural orthostatic tachycardia syndrome in patients suffering from orthostatic intolerance: A combined form of autonomic dysfunction[J]. Pacing Clin Electrophysiol, 2011, 34 (5): 549- 554.
doi: 10.1111/j.1540-8159.2010.02994.x |
| 22 |
Tao C , Jin H , Du J . Management of orthostatic intolerance in children: the state of the art[J]. World J Pediatr, 2020, 16 (6): 543- 548.
doi: 10.1007/s12519-019-00329-0 |
| 23 |
Kaufmann H , Norcliffe-Kaufmann L , Palma JA . Baroreflex dysfunction[J]. N Engl J Med, 2020, 382 (2): 163- 178.
doi: 10.1056/NEJMra1509723 |
| 24 |
Iacoviello M , Guida P , Forleo C , et al. Impaired arterial baroreflex function before nitrate-induced vasovagal syncope during head-up tilt test[J]. Europace, 2008, 10 (10): 1170- 1175.
doi: 10.1093/europace/eun217 |
| 25 | 肖要, 张小华, 魏红芳, 等. 儿童直立不耐受发病机制研究进展[J]. 兰州大学学报(医学版), 2021, 47 (6): 82- 88. |
| 26 |
Mitro P , Mudráková K , Micková H , et al. Hemodynamic parameters and heart rate variability during a tilt test in relation to gene polymorphism of renin-angiotensin and serotonin system[J]. Pacing Clin Electrophysiol, 2008, 31 (12): 1571- 1580.
doi: 10.1111/j.1540-8159.2008.01228.x |
| 27 |
Stewart JM , Medow MS , Sutton R , et al. Mechanisms of vasovagal syncope in the young: reduced systemic vascular resistance versus reduced cardiac output[J]. J Am Heart Assoc, 2017, 6 (1): e004417.
doi: 10.1161/JAHA.116.004417 |
| 28 |
Bai W , Chen S , Jin H , et al. Vascular dysfunction of postural tachycardia syndrome in children[J]. World J Pediatr, 2018, 14 (1): 13- 17.
doi: 10.1007/s12519-017-0104-8 |
| 29 |
Mosqueda-Garcia R , Furlan R , Tank J , et al. The elusive pathophysiology of neurally mediated syncope[J]. Circulation, 2000, 102 (23): 2898- 2906.
doi: 10.1161/01.CIR.102.23.2898 |
| 30 |
Liao Y , Du J . Pathophysiology and individualized management of vasovagal syncope and postural tachycardia syndrome in children and adolescents: An update[J]. Neurosci Bull, 2020, 36 (6): 667- 681.
doi: 10.1007/s12264-020-00497-4 |
| [1] | 李宗瀚, 黄洋阅, 李宁, 李明磊, 宋宏程, 张潍平, 刘超. 国产单孔蛇形臂机器人手术系统在儿童肾盂成形术中的应用[J]. 北京大学学报(医学版), 2025, 57(4): 662-665. |
| [2] | 赵兆, 张维宇, 杨文博, 张勇杰, 张晓鹏, 赵慧颖, 周刚, 王强. 低龄、低体重儿童肾移植2例[J]. 北京大学学报(医学版), 2025, 57(4): 803-807. |
| [3] | 张依航, 蔡珊, 陈子玥, 刘云飞, 党佳佳, 师嫡, 李佳欣, 黄天彧, 宋逸. 基于RE-AIM框架儿童青少年近视与肥胖共病综合干预实施性研究结局指标的构建[J]. 北京大学学报(医学版), 2025, 57(3): 436-441. |
| [4] | 唐孟利, 刘扬, 秦冉, 郭欣, 李宏田. 我国10省幼儿园5~6岁儿童近视和近视前期流行特征[J]. 北京大学学报(医学版), 2025, 57(3): 442-447. |
| [5] | 刘光旭, 张良, 赵厚宇, 邓思危, 杨君婷, 李宁, 马瑞, 何艳, 许国章, 刘志科, 詹思延. 2015—2021年宁波市6岁以下儿童热性惊厥的流行病学特征[J]. 北京大学学报(医学版), 2025, 57(3): 584-591. |
| [6] | 李琳, 廖津津. 应用ROC曲线评估久坐行为对儿童青少年视力不良的预测价值[J]. 北京大学学报(医学版), 2025, 57(3): 614-619. |
| [7] | 王紫薇, 李闵, 高慧, 邓芳. 链球菌感染与过敏性紫癜肾炎患儿肾损害的相关性[J]. 北京大学学报(医学版), 2025, 57(2): 284-290. |
| [8] | 邓敏婷, 王楠, 夏斌, 赵玉鸣, 朱俊霞. 儿童及青少年挫入恒前牙自行再萌出的相关影响因素[J]. 北京大学学报(医学版), 2025, 57(1): 148-153. |
| [9] | 杨颖婷, 李若竹, 窦桂丽, 雷玥, 夏斌. iRoot BP Plus用于年轻恒牙外伤部分牙髓切断治疗的临床随机对照研究[J]. 北京大学学报(医学版), 2024, 56(6): 1083-1088. |
| [10] | 赵双云, 邹思雨, 李雪莹, 沈丽娟, 周虹. 中文版口腔健康素养量表简版(HeLD-14)在学龄前儿童家长中应用的信度和效度评价[J]. 北京大学学报(医学版), 2024, 56(5): 828-832. |
| [11] | 陈心心, 唐哲, 乔艳春, 荣文笙. 北京市密云区4岁儿童患龋状况及其与龋活跃性检测的相关性[J]. 北京大学学报(医学版), 2024, 56(5): 833-838. |
| [12] | 岳芷涵,韩娜,鲍筝,吕瑾莨,周天一,计岳龙,王辉,刘珏,王海俊. 儿童早期体重指数轨迹与超重风险关联的前瞻性队列研究[J]. 北京大学学报(医学版), 2024, 56(3): 390-396. |
| [13] | 费秀文,刘斯,汪波,董爱梅. 成人及儿童组织坏死性淋巴结炎临床特征及治疗[J]. 北京大学学报(医学版), 2024, 56(3): 533-540. |
| [14] | 俞光岩. 儿童唾液腺疾病[J]. 北京大学学报(医学版), 2024, 56(1): 1-3. |
| [15] | 闫晓晋,刘云飞,马宁,党佳佳,张京舒,钟盼亮,胡佩瑾,宋逸,马军. 《中国儿童发展纲要(2011-2020年)》实施期间中小学生营养不良率变化及其政策效应分析[J]. 北京大学学报(医学版), 2023, 55(4): 593-599. |
|
||
