北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (6): 1106-1111. doi: 10.19723/j.issn.1671-167X.2022.06.008
系统性红斑狼疮合并视网膜病变的临床及免疫学特点
李敏1,侯林卿1,2,金月波1,何菁1,*( )
)
- 1. 北京大学人民医院风湿免疫科,北京 100044
2. 临汾市第三人民医院风湿免疫科,山西临汾 041000
Clinical and immunological characteristics of systemic lupus erythematosus with retinopathy
Min LI1,Lin-qing HOU1,2,Yue-bo JIN1,Jing HE1,*()
- 1. Department of Rheumatology and Immunology, Peking University People's Hospital, Bejing 100044, China
2. Department of Rheumatology and Immunology, The Third People's Hospital of Linfen, Linfen 041000, Shanxi, China
摘要:
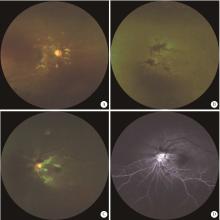
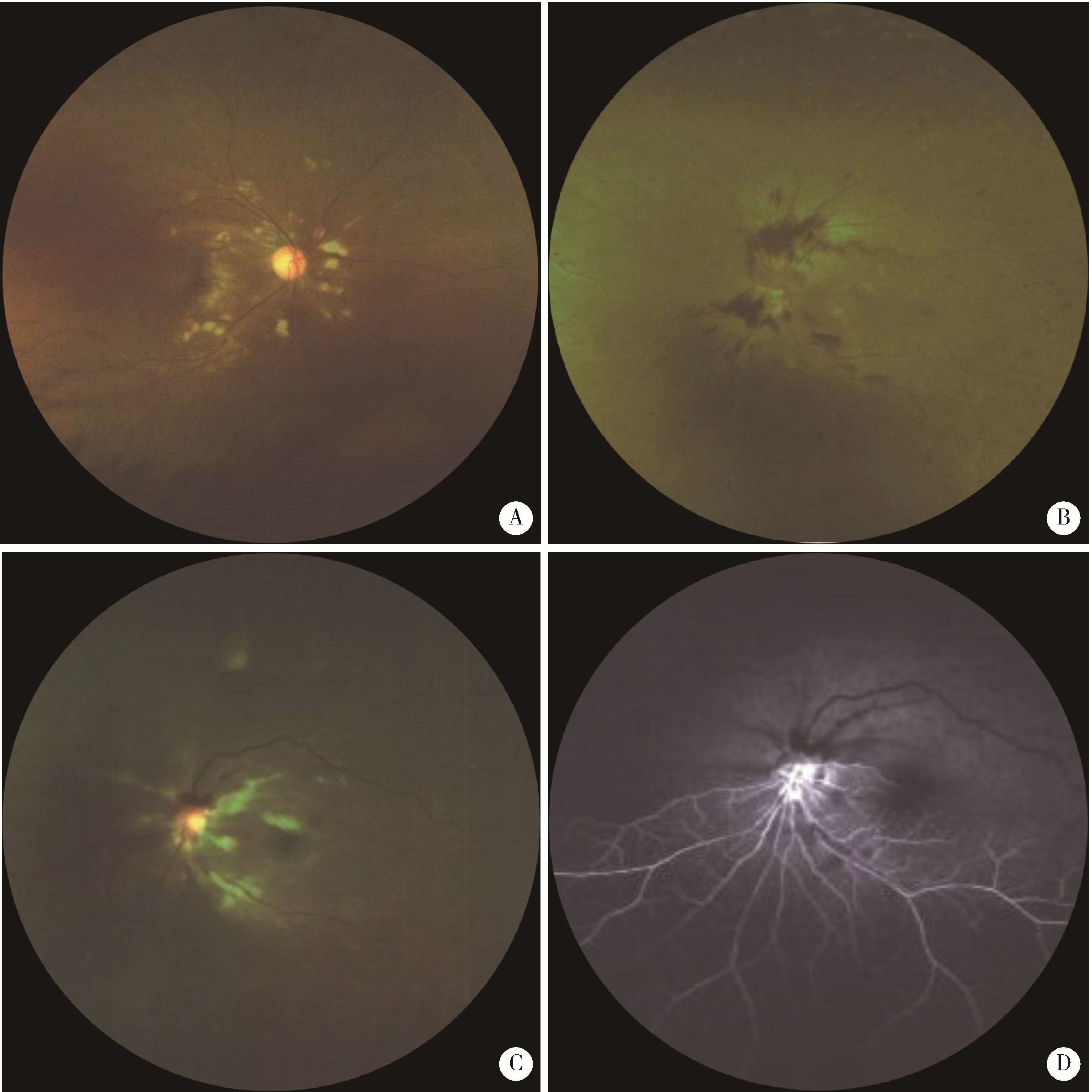
目的: 探讨系统性红斑狼疮(systemic lupus erythematosus, SLE)合并视网膜病变的临床及免疫学特点。方法: 选择2009年1月至2022年7月于北京大学人民医院住院的无高血压无糖尿病的SLE合并视网膜病变患者50例(眼病组),按性别、年龄匹配病程中无视物模糊症状及眼底检查没有视网膜病变的SLE患者50例(非眼病组),对两组患者的临床表现、实验室检查及淋巴细胞亚群进行分析。结果: 眼病组患者最常见的眼底表现为棉絮斑(33/50,66.0%),其次是视网膜出血(31/50,62.0%)。视网膜病变可发生在SLE病程的任何阶段,中位时间为1年(病程范围为20 d至30年)。眼病组出现狼疮性肾炎比例(72.0% vs. 46.0%, P=0.008)和浆膜炎比例(58.0% vs. 28.0%, P=0.002)显著高于非眼病组。眼病组同时出现神经精神性狼疮(neuropsychiatric systemic lupus erythematosus, NPSLE)比例较非眼病组升高,但差异无统计学意义。与非眼病组相比,眼病组中抗心磷脂抗体阳性比例(30.0% vs. 12.0%, P=0.027)、系统性红斑狼疮疾病活动指数评分(中位数22.0 vs. 10.5, P < 0.001)、红细胞沉降率(P < 0.001),C反应蛋白水平(P=0.019)和24 h尿蛋白定量(P=0.026)均显著升高,血红蛋白水平明显减低[(91.64±25.18) g/L vs. (113.96±18.57) g/L, P < 0.001]。与非眼病组相比,SLE视网膜病变患者外周血CD19+B细胞比例显著升高(P=0.010),CD4+T细胞比例明显减低(P=0.025),自然杀伤(natural killer,NK)细胞比例减低(P=0.051)。结论: SLE视网膜病变提示更高的SLE疾病活动性,更易合并肾脏系统、血液系统等损害,建议对所有SLE患者尽早进行眼底筛查。SLE视网膜病变患者可能存在更显著的B细胞异常增殖,应给予积极治疗以防止其他重要脏器受累。
中图分类号:
- R593.24

| 1 |
Au A , O'Day J . Review of severe vaso-occlusive retinopathy in systemic lupus erythematosus and the antiphospholipid syndrome: Associations, visual outcomes, complications and treatment[J]. Clin Exp Ophthalmol, 2004, 32 (1): 87- 100.
doi: 10.1046/j.1442-9071.2004.00766.x |
| 2 |
Moulton VR , Suarez-Fueyo A , Meidan E , et al. Pathogenesis of human systemic lupus erythematosus: A cellular perspective[J]. Trends Mol Med, 2017, 23 (7): 615- 635.
doi: 10.1016/j.molmed.2017.05.006 |
| 3 |
Dammacco R , Procaccio P , Racanelli V , et al. Ocular involvement in systemic lupus erythematosus: The experience of two tertiary referral centers[J]. Ocul Immunol Inflamm, 2018, 26 (8): 1154- 1165.
doi: 10.1080/09273948.2018.1501495 |
| 4 |
Yen YC , Weng SF , Chen HA , et al. Risk of retinal vein occlusion in patients with systemic lupus erythematosus: A population-based cohort study[J]. Br J Ophthalmol, 2013, 97 (9): 1192- 1196.
doi: 10.1136/bjophthalmol-2013-303265 |
| 5 |
Lanham JG , Barrie T , Kohner EM , et al. SLE retinopathy: Evaluation by fluorescein angiography[J]. Ann Rheum Dis, 1982, 41 (5): 473- 478.
doi: 10.1136/ard.41.5.473 |
| 6 | Hochberg MC . Updating the American college of rheumatology revised criteria for the classification of systemic lupus erythematosus[J]. Arthritis Rheum, 1997, 40 (9): 1725. |
| 7 | Gladman DD , Ibanez D , Urowitz MB . Systemic lupus erythematosus disease activity index 2000[J]. J Rheumatol, 2002, 29 (2): 288- 291. |
| 8 |
Md Noh UK , Zahidin AZA , Yong TK . Retinal vasculitis in systemic lupus erythematosus: An indication of active disease[J]. Clinics and Practice, 2012, 2 (2): 54.
doi: 10.4081/cp.2012.e54 |
| 9 |
Stafford-Brady FJ , Urowitz MB , Gladman DD , et al. Lupus retinopathy. Patterns, associations, and prognosis[J]. Arthritis Rheum, 1988, 31 (9): 1105- 1110.
doi: 10.1002/art.1780310904 |
| 10 |
Giorgi D , Pace F , Giorgi A , et al. Retinopathy in systemic lupus erythematosus: Pathogenesis and approach to therapy[J]. Hum Immunol, 1999, 60 (8): 688- 696.
doi: 10.1016/S0198-8859(99)00035-X |
| 11 |
D'Cruz D . Vasculitis in systemic lupus erythematosus[J]. Lupus, 1998, 7 (4): 270- 274.
doi: 10.1191/096120398678920082 |
| 12 |
Kharel R , Shah DN , Singh D . Role of lupus retinopathy in systemic lupus erythematosus[J]. Ophthalmic Inflamm Infect, 2016, 6 (1): 1- 4.
doi: 10.1186/s12348-015-0068-6 |
| 13 |
Seth G , Chengappa KG , Misra DP , et al. Lupus retinopathy: A marker of active systemic lupus erythematosus[J]. Rheum Int, 2018, 38 (8): 1495- 1501.
doi: 10.1007/s00296-018-4083-4 |
| 14 |
曹绪胜, 纪海霞, 张永鹏, 等. 全身使用糖皮质激素继发中心性浆液性脉络膜视网膜病变的临床特征[J]. 眼科, 2020, 29 (3): 193- 197.
doi: 10.3969/j.issn.1006-8422.2020.03.001 |
| 15 |
Million M , Raoult D . The pathogenesis of the antiphospholipid syndrome[J]. N Engl J Med, 2013, 368 (24): 2335.
doi: 10.1056/NEJMc1300484 |
| 16 |
Jeon S , Lee WK . Aggravated capillary non-perfusion after intravitreal bevacizumab for macular edema secondary to systemic lupus erythematosus and anti-phospholipid syndrome[J]. Lupus, 2012, 21 (3): 335- 337.
doi: 10.1177/0961203311422095 |
| 17 | Zhu W , Wu Y , Xu M , et al. Correction: Antiphospholipid antibody and risk of retinal vein occlusion: A systematic review and meta-analysis[J]. PLoS One, 2016, 11 (6): e157536. |
| 18 |
Lipsky PE . Systemic lupus erythematosus: An autoimmune disease of B cell hyperactivity[J]. Nat Immunol, 2001, 2 (9): 764- 766.
doi: 10.1038/ni0901-764 |
| 19 |
Wei C , Anolik J , Cappione A , et al. A new population of cells lacking expression of CD27 represents a notable component of the B cell memory compartment in systemic lupus erythematosus[J]. J Immunol, 2007, 178 (10): 6624- 6633.
doi: 10.4049/jimmunol.178.10.6624 |
| 20 |
Hickman RA , Denniston AK , Yee CS , et al. Bilateral retinal vasculitis in a patient with systemic lupus erythematosus and its remission with rituximab therapy[J]. Lupus, 2010, 19 (3): 327- 329.
doi: 10.1177/0961203309347332 |
| 21 |
Damato E , Chilov M , Lee R , et al. Plasma exchange and rituximab in the management of acute occlusive retinal vasculopathy secondary to systemic lupus erythematosus[J]. Ocul Immunol Inflamm, 2011, 19 (5): 379- 381.
doi: 10.3109/09273948.2011.603069 |
| 22 |
Tselios K , Lam WC , Urowitz MB , et al. Rituximab for sight-threatening lupus-related retinal vasculitis[J]. J Clin Rheumatol, 2018, 24 (2): 93- 94.
doi: 10.1097/RHU.0000000000000600 |
| 23 |
Liu M , Liu J , Zhang X , et al. Activation status of CD56(dim) natural killer cells is associated with disease activity of patients with systemic lupus erythematosus[J]. Clin Rheumatol, 2021, 40 (3): 1103- 1112.
doi: 10.1007/s10067-020-05306-x |
| [1] | 赵豆豆, 齐晅, 黄博, 高伟波, 裴源源, 金月波, 邵苗, 何菁. 感染性肺炎与免疫相关间质性肺病中淋巴细胞亚群的表达[J]. 北京大学学报(医学版), 2026, 58(3): 624-630. |
| [2] | 马豆豆, 马晓彩, 常天静, 王丽芳, 丁艳, 石连杰. 临床表现似系统性红斑狼疮的大B细胞淋巴瘤骨髓受累1例[J]. 北京大学学报(医学版), 2026, 58(3): 666-669. |
| [3] | 汤晓菲, 丁秋玲, 张阳, 王育梅, 田美伊, 孙卓, 王荣荣, 陈妍, 刘坚. 阿伐曲泊帕治疗难治性系统性红斑狼疮相关血小板减少1例[J]. 北京大学学报(医学版), 2026, 58(2): 405-409. |
| [4] | 林文灏, 谢阳, 王芳晴, 王淑盈, 刘香君, 胡凡磊, 贾园. 基于B细胞单细胞转录组测序的干燥综合征分子分型[J]. 北京大学学报(医学版), 2025, 57(6): 1032-1041. |
| [5] | 李欣艺, 赵金霞, 穆荣. 阿司匹林对系统性红斑狼疮妊娠者结局的影响[J]. 北京大学学报(医学版), 2025, 57(6): 1074-1080. |
| [6] | 王晓林, 郭邵逸, 陈大召, 温锡杰, 华勇, 张亮, 张秦. 全髋关节置换术治疗系统性红斑狼疮继发股骨头缺血性坏死的随访研究[J]. 北京大学学报(医学版), 2025, 57(6): 1081-1088. |
| [7] | 卫春, 杨月, 赵新菊, 刘栩, 贾园. 系统性红斑狼疮合并自身免疫性郎飞结病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1174-1179. |
| [8] | 赵凯, 鲁芙爱, 王永福. 中枢神经系统感染模拟神经精神狼疮1例[J]. 北京大学学报(医学版), 2025, 57(6): 1188-1192. |
| [9] | 王小梦, 曾晓君, 李娟. 黎族与汉族系统性红斑狼疮患者的主要临床特征[J]. 北京大学学报(医学版), 2025, 57(6): 1213-1218. |
| [10] | 王文琼, 侯玉珂, 李春, 张学武. 系统性红斑狼疮患者不良妊娠结局的预测因素[J]. 北京大学学报(医学版), 2025, 57(3): 599-603. |
| [11] | 王红彦, 李鑫铭, 房柯池, 朱华群, 贾汝琳, 王晶. 系统性红斑狼疮疾病活动度相关特征分析及评估模型的构建[J]. 北京大学学报(医学版), 2024, 56(6): 1017-1022. |
| [12] | 陈丹丹, 李云, 卢情怡, 相晓红, 孙峰, 李英妮, 赵静, 王红彦, 李春. 育龄期系统性红斑狼疮患者卵巢功能的评价及其影响因素[J]. 北京大学学报(医学版), 2024, 56(6): 1023-1028. |
| [13] | 王莉, 高超, 任欢欢, 沈艳平, 黄晓玮, 姚鸿, 韩丹丹. 系统性红斑狼疮患者自我管理能力现状及相关因素分析[J]. 北京大学学报(医学版), 2024, 56(6): 1029-1035. |
| [14] | 柴静, 王钥, 穆荣, 赵金霞. 系统性红斑狼疮累及穹窿柱导致低钠血症1例[J]. 北京大学学报(医学版), 2024, 56(6): 1115-1118. |
| [15] | 王明霞, 丁菱, 王敏, 邹婵娟, 颜丝语, 梁颖文, 王伟佳, 何善智. 双靶点嵌合抗原受体T细胞治疗系统性红斑狼疮患者停药后安全孕产1例[J]. 北京大学学报(医学版), 2024, 56(6): 1119-1125. |
|
||
