北京大学学报(医学版) ›› 2023, Vol. 55 ›› Issue (6): 1045-1052. doi: 10.19723/j.issn.1671-167X.2023.06.014
未分化结缔组织病患者的妊娠结局、疾病演变及其影响因素
游芳凝1,2,罗靓3,刘香君1,张学武1,李春1,*( )
)
- 1. 北京大学人民医院风湿免疫科, 北京 100044
2. 重庆市中医院肾病风湿免疫科, 重庆 400011
3. 重庆市渝北区人民医院中医科, 重庆 401120
Analysis of pregnancy outcomes, disease progression, and risk factors in patients with undifferentiated connective tissue disease
Fang-ning YOU1,2,Liang LUO3,Xiang-jun LIU1,Xue-wu ZHANG1,Chun LI1,*()
- 1. Department of Rheumatology and Immunology, Peking University People's Hospital, Beijing 100044, China
2. Department of Nephropathy and Rheumatology, Chongqing Hospital of Traditional Chinese Medicine, Chongqing 400011, China
3. Department of Chinese Medicine, the People's Hospital of Yubei District of Chongqing City, Chongqing 401120, China
摘要:
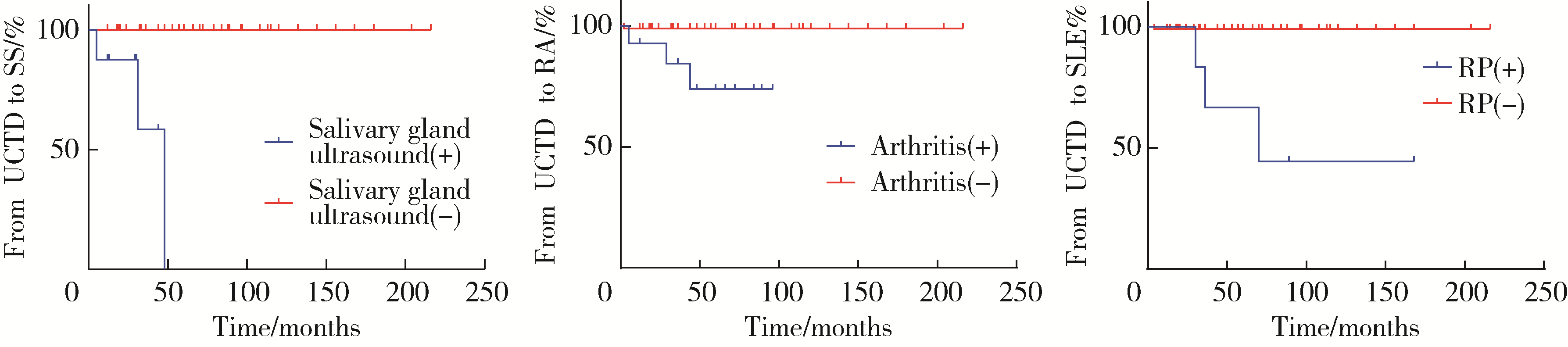
目的: 研究未分化结缔组织病(undifferentiated connective tissue disease, UCTD)患者的妊娠结局、疾病演变及其影响因素。方法: 选择2009年1月至2022年8月在北京大学人民医院就诊并且符合UCTD分类标准孕妇的病例资料进行回顾性分析; 106例UCTD孕妇根据妊娠结局分为不良妊娠结局组(adverse pregnancy outcomes, APOs)(53例)和无APOs组(53例), 比较两组患者临床表现、实验室指标及妊娠结局的差异。不良妊娠结局包括流产、早产、子痫前期、胎膜早破(premature rupture of membranes, PROM)、宫内生长受限(intrauterine growth restriction, IUGR)、产后出血(postpartum hemorrhage, PPH)、死胎、小于胎龄儿(small for gestational age infant, SGA)、低出生体质量(low birth weight infant, LBW)、出生缺陷。采用Logistic回归分析不良妊娠结局的危险因素, 使用Kaplan-Meier法进行生存分析, 通过Cox回归分析筛选出UCTD演变为明确CTD的危险因素。结果: 在106例UCTD患者中, 99例(93.39%)为活产, 4例(3.77%)死胎, 3例(2.83%)流产, 20例(18.86%)早产, 6例(5.66%)SGA, 17例(16.03%)LBW, 11例(10.37%)子痫前期, 7例(6.60%)IUGR, 19例(17.92%)PROM, 10例(9.43%)PPH。APOs组抗SSA抗体阳性率较无APOs组更高(73.58% vs. 54.71%, P=0.036), 白细胞减少比例更高(15.09% vs. 3.77%, P=0.046), 血红蛋白水平较无APOs组明显降低[109.00 (99.50, 118.00) g/L vs. 124.00 (111.50, 132.00) g/L, P < 0.001]。多因素Logistic回归分析显示白细胞减少(OR=0.827, 95%CI: 0.688~0.994)是UCTD患者发生APOs的独立危险因素(P=0.042)。15例(14.15%)UCTD在平均随访5.00(3.00, 7.00)年内演变为明确的结缔组织病, 其中干燥综合征8例(7.54%), 系统性红斑狼疮(systemic lupus erythematosus, SLE)4例(3.77%), 类风湿关节炎4例(3.77%), 混合性结缔组织病1例(0.94%)。雷诺现象(Raynaud phenomenon, RP) (HR=40.157, 95%CI: 3.172~508.326)是UCTD患者妊娠期及产后演变为SLE的独立危险因素(P=0.003)。结论: 白细胞减少是UCTD患者发生APOs的独立危险因素, 雷诺现象是UCTD患者演变为SLE的独立危险因素, 严格的疾病监测、定期随访是预防UCTD合并妊娠患者发生不良妊娠结局和预测疾病演变的关键措施。
中图分类号:
- R593.2

| 1 |
Mosca M , Tani C , Neri C , et al. Undifferentiated connective tissue diseases (UCTD)[J]. Autoimm Rev, 2006, 6 (1): 1- 4.
doi: 10.1016/j.autrev.2006.03.004 |
| 2 | García-González M , Rodríguez-Lozano B , Bustabad S , et al. Undifferentiated connective tissue disease: Predictors of evolution into definite disease[J]. Clin Exp Rheumatol, 2017, 35 (5): 739- 745. |
| 3 |
Mecacci F , Pieralli A , Bianchi B , et al. The impact of autoimmune disorders and adverse pregnancy outcome[J]. Semin Perinatol, 2007, 31 (4): 223- 226.
doi: 10.1053/j.semperi.2007.05.005 |
| 4 | Mosca M , Neri R , Bombardieri S . Undifferentiated connective tissue diseases (UCTD): A review of the literature and a proposal for preliminary classification criteria[J]. Clin Exp Rheumatol, 1999, 17 (5): 615- 620. |
| 5 |
Practice Committee of the American Society for Reproductive Medicine . Evaluation and treatment of recurrent pregnancy loss: A committee opinion[J]. Fertil Steril, 2012, 98 (5): 1103- 1111.
doi: 10.1016/j.fertnstert.2012.06.048 |
| 6 |
Vogel JP , Chawanpaiboon S , Moller AB , et al. The global epidemiology of preterm birth[J]. Best Pract Res Clin Obstet Gynaecol, 2018, 52, 3- 12.
doi: 10.1016/j.bpobgyn.2018.04.003 |
| 7 | Tyas BD , Lestari P , Akbar MIA . Maternal perinatal outcomes related to advanced maternal age in preeclampsia pregnant women[J]. J Family Reprod Health, 2019, 13 (4): 191- 200. |
| 8 |
Sharma D , Shastri S , Farahbakhsh N , et al. Intrauterine growth restriction: Part 1[J]. J Matern Fetal Neonatal Med, 2016, 29 (24): 3977- 3987.
doi: 10.3109/14767058.2016.1152249 |
| 9 |
American College of Obstetricians and Gynecologists' Committee on Practice Bulletins-Obstetrics . Practice bulletin No.172: Premature rupture of membranes[J]. Obstet Gynecol, 2016, 128 (4): 165- 177.
doi: 10.1097/AOG.0000000000001712 |
| 10 | Sheldon WR , Blum J , Vogel JP , et al. Postpartum haemorrhage management, risks, and maternal outcomes: Findings from the World Health Organization Multicountry Survey on Maternal and Newborn Health[J]. BJOG, 2014, 121 (Suppl 1): 5- 13. |
| 11 |
Robinson GE . Pregnancy loss[J]. Best Pract Res Clin Obstet Gynaecol, 2014, 28 (1): 169- 178.
doi: 10.1016/j.bpobgyn.2013.08.012 |
| 12 |
Bertino E , Spada E , Occhi L , et al. Neonatal anthropometric charts: The Italian neonatal study compared with other European studies[J]. J Pediatr Gastroenterol Nutr, 2010, 51 (3): 353- 361.
doi: 10.1097/MPG.0b013e3181da213e |
| 13 |
Krasevec J , Blencowe H , Coffey C , et al. Study protocol for UNICEF and WHO estimates of global, regional, and national low birthweight prevalence for 2000 to 2020[J]. Gates Open Res, 2022, 6, 80- 93.
doi: 10.12688/gatesopenres.13666.1 |
| 14 | World Health Organization (WHO). Sixty-third world health assembly. Birth defects[R]. Geneva: WHO, 2010. |
| 15 |
Ostensen M , Andreoli L , Brucato A , et al. State of the art: Reproduction and pregnancy in rheumatic diseases[J]. Autoimmun Rev, 2015, 14 (5): 376- 386.
doi: 10.1016/j.autrev.2014.12.011 |
| 16 |
Goldenberg RL , Culhane JF , Iams JD , et al. Epidemiology and causes of preterm birth[J]. Lancet, 2008, 371 (9606): 75- 84.
doi: 10.1016/S0140-6736(08)60074-4 |
| 17 |
Radin M , Schreiber K , Cecchi I , et al. A Multicentre study of 244 pregnancies in undifferentiated connective tissue disease: Maternal/fetal outcomes and disease evolution[J]. Rheumatology (Oxford), 2020, 59 (9): 2412- 2418.
doi: 10.1093/rheumatology/kez620 |
| 18 |
Muñoz Muñoz1 C , Ahmed K , Thomas M , et al. Comparing pregnancy outcomes in patients with criteria and non-criteria autoimmune disease: A systematic review[J]. Lupus, 2022, 31 (1): 5- 18.
doi: 10.1177/09612033211061850 |
| 19 |
Haase I , Fischer-Betz R . State of the art: Fertility and pregnancy in rheumatic diseases[J]. Z Rheumatol, 2021, 80 (8): 699- 706.
doi: 10.1007/s00393-021-01073-5 |
| 20 |
Luo L , Li XR , Li C , et al. Risk factors for adverse pregnancy outcomes in women with rheumatoid arthritis and follow-up of their offspring[J]. Clin Rheumatol, 2022, 41 (10): 3135- 3141.
doi: 10.1007/s10067-022-06233-9 |
| 21 |
Erden A , Apaydın H , Fanouriakis A , et al. Performance of the systemic lupus erythematosus risk probability index in a cohort of undifferentiated connective tissue disease[J]. Rheumatology (Oxford), 2022, 61 (9): 3606- 3613.
doi: 10.1093/rheumatology/keac005 |
| 22 |
张晓英, 温鸿雁, 陈俊伟, 等. 未分化结缔组织病合并骨髓增生异常综合征1例[J]. 北京大学学报(医学版), 2012, 44 (2): 316- 319.
doi: 10.3969/j.issn.1671-167X.2012.02.033 |
| 23 |
Lin L , Wei Y , Zhu W , et al. Prevalence, risk factors and associated adverse pregnancy outcomes of anaemia in Chinese pregnant women: A multicentre retrospective study[J]. BMC Pregnancy Childbirth, 2018, 18 (1): 111- 118.
doi: 10.1186/s12884-018-1739-8 |
| 24 |
Li M , Huang SJ . Innate immunity, coagulation and placenta related adverse pregnancy outcomes[J]. Thromb Res, 2009, 124 (6): 656- 662.
doi: 10.1016/j.thromres.2009.07.012 |
| 25 | 孔德璇, 张志坤, 李慧东. 系统性红斑狼疮与孕产妇不良妊娠结局的相关性[J]. 中国妇幼保健, 2022, 37 (10): 1865- 1868. |
| 26 |
Klein A , Molad Y . Hematological manifestations among patients with rheumatic diseases[J]. Acta Haematol, 2021, 144 (4): 403- 412.
doi: 10.1159/000511759 |
| 27 |
Wang F , Jia W , Fan M , et al. Single cell immune landscape of human recurrent miscarriage[J]. Genomics Proteomics Bioinformatics, 2021, 19 (2): 208- 222.
doi: 10.1016/j.gpb.2020.11.002 |
| 28 | Cavazzana I , Franceschini F , Belfiore N , et al. Undifferentiated connective tissue disease with antibodies to Ro/SSa: Clinical features and follow-up of 148 patients[J]. Clin Exp Rheumatol, 2001, 19 (4): 403- 409. |
| 29 |
Tektonidou MG , Andreoli L , Limper M , et al. EULAR recommendations for the management of antiphospholipid syndrome in adults[J]. Ann Rheum Dis, 2019, 78 (10): 1296- 1304.
doi: 10.1136/annrheumdis-2019-215213 |
| 30 |
Duan JN , Ma D , Wen XT , et al. Hydroxychloroquine prophylaxis for preeclampsia, hypertension and prematurity in pregnant patients with systemic lupus erythematosus: A meta-analysis[J]. Lupus, 2021, 30 (7): 1163- 1174.
doi: 10.1177/09612033211007199 |
| [1] | 魏慧, 张警丰, 姚中强, 赵金霞. 类风湿关节炎合并慢性病贫血患者的临床特征及相关因素[J]. 北京大学学报(医学版), 2026, 58(2): 307-312. |
| [2] | 赵杰, 付春, 赵秀娟, 薛海岩, 李纾, 王振洲, 朱凤雪. 胸部创伤患者在重症监护病房内发生呼吸机相关性肺炎的危险因素[J]. 北京大学学报(医学版), 2026, 58(2): 351-358. |
| [3] | 郭芷均, 俎明, 马超, 张贺军, 张静, 丁士刚. 同时性多发早期胃癌漏诊病灶的临床病理特征[J]. 北京大学学报(医学版), 2026, 58(2): 410-415. |
| [4] | 李博闻, 张强, 孙益鑫. 儿童及青年漏斗胸患者Nuss术后发生脊柱侧弯的风险预测模型建立及验证[J]. 北京大学学报(医学版), 2025, 57(5): 941-946. |
| [5] | 杨小勇, 张帆, 马潞林, 刘承. 前列腺导管腺癌临床特征及腺外侵犯的影响因素[J]. 北京大学学报(医学版), 2025, 57(5): 956-960. |
| [6] | 刘伟, 郭稳, 过哲, 李春艳, 李云龙, 刘思奇, 张亮, 宋慧. 痛风患者放射学阴性骨侵蚀的相关危险因素[J]. 北京大学学报(医学版), 2025, 57(4): 735-739. |
| [7] | 陆梦溪, 刘秋萍, 周恬静, 刘晓非, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 基于社区人群队列的甘油三酯-葡萄糖指数与心血管病发病和死亡的关联[J]. 北京大学学报(医学版), 2025, 57(3): 430-435. |
| [8] | 杨树涵, 李奕昕, 崔浩亮, 王佑新, 吴玉莹, 王明月, 杨依凡, 恩卡尔·努尔, 杨磊, 王辉. 代谢相关脂肪性肝病及其心脏代谢风险指标异常与不良妊娠结局的相关性[J]. 北京大学学报(医学版), 2025, 57(3): 487-495. |
| [9] | 杨龙傲, 金旭, 黄文初, 何丽华, 陈娟. 视屏作业人员视疲劳及干眼的流行病学调查[J]. 北京大学学报(医学版), 2025, 57(3): 554-561. |
| [10] | 王文琼, 侯玉珂, 李春, 张学武. 系统性红斑狼疮患者不良妊娠结局的预测因素[J]. 北京大学学报(医学版), 2025, 57(3): 599-603. |
| [11] | 郭华秋, 王哲, 杨雪, 白洁. 口腔急诊出血患者的临床特征与危险因素[J]. 北京大学学报(医学版), 2025, 57(1): 142-147. |
| [12] | 邓敏婷, 王楠, 夏斌, 赵玉鸣, 朱俊霞. 儿童及青少年挫入恒前牙自行再萌出的相关影响因素[J]. 北京大学学报(医学版), 2025, 57(1): 148-153. |
| [13] | 李钰锴, 王红彦, 罗靓, 李云, 李春. 抗磷脂抗体在白塞病合并血栓中的临床意义[J]. 北京大学学报(医学版), 2024, 56(6): 1036-1040. |
| [14] | 田杨, 韩永正, 李娇, 王明亚, 曲音音, 房景超, 金辉, 李民, 王军, 徐懋, 王圣林, 郭向阳. 颈椎前路手术后硬膜外血肿的发生率和危险因素[J]. 北京大学学报(医学版), 2024, 56(6): 1058-1064. |
| [15] | 王明瑞, 赖金惠, 姬家祥, 唐鑫伟, 胡浩浦, 王起, 许克新, 徐涛, 胡浩. 使用中文版威斯康星结石生活质量问卷预测肾结石患者生活质量降低的危险因素[J]. 北京大学学报(医学版), 2024, 56(6): 1069-1074. |
|
||
