北京大学学报(医学版) ›› 2024, Vol. 56 ›› Issue (4): 661-666. doi: 10.19723/j.issn.1671-167X.2024.04.019
具有低度恶性潜能的多房囊性肾肿瘤的临床病理特征及预后
虞乐,邓绍晖,张帆,颜野,叶剑飞,张树栋*( )
)
- 北京大学第三医院泌尿外科,北京 100191
Clinicopathological characteristics and prognosis of multilocular cystic renal neoplasm of low malignant potential
Le YU,Shaohui DENG,Fan ZHANG,Ye YAN,Jianfei YE,Shudong ZHANG*()
- Department of Urology, Peking University Third Hospital, Beijing 100191, China
摘要:
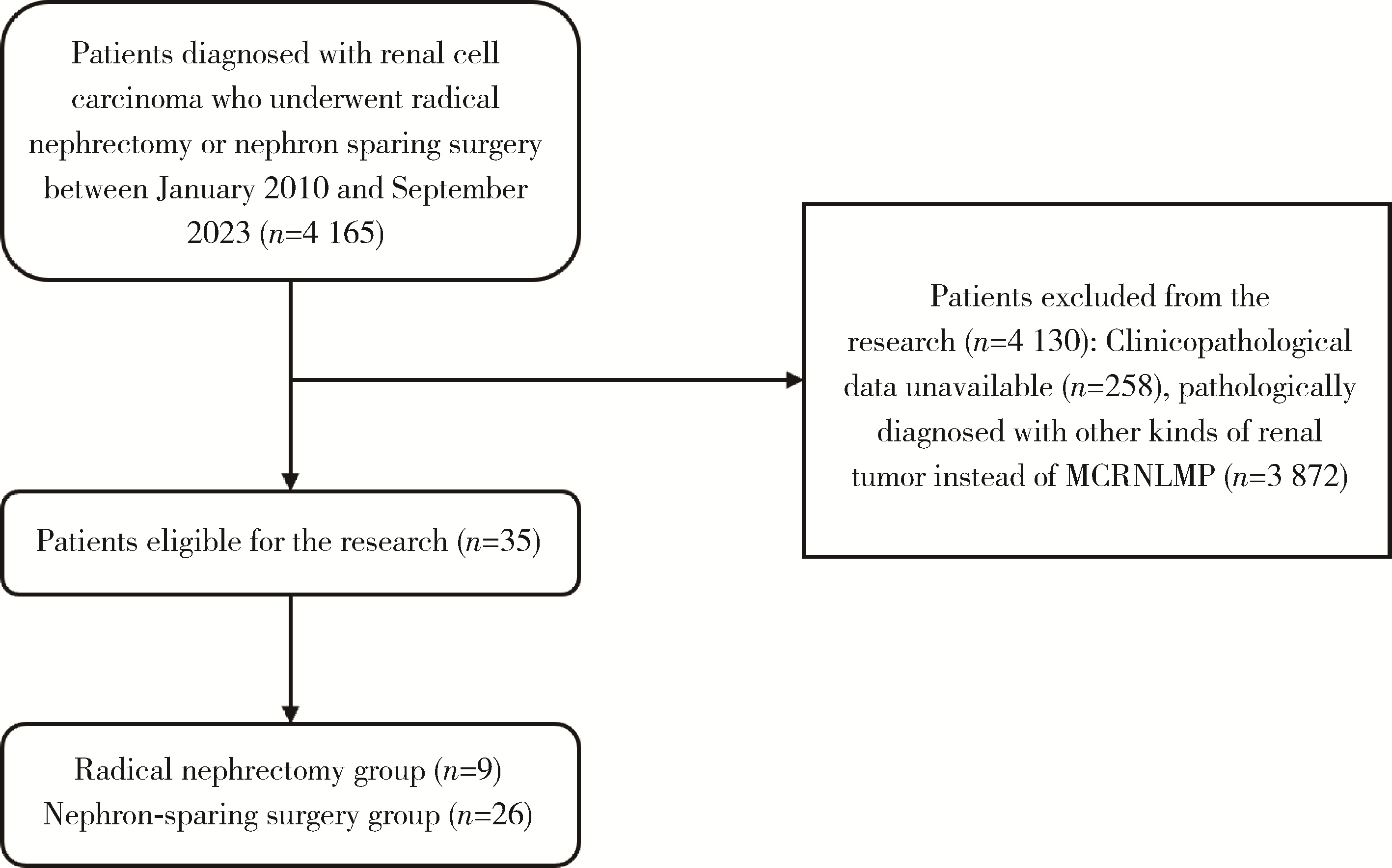
目的: 分析具有低度恶性潜能的多房囊性肾肿瘤(multilocular cystic renal neoplasm of low malignant potential, MCRNLMP)患者的临床病理特征与预后,对比接受不同手术方式的具有低度恶性潜能的多房囊性肾肿瘤患者的临床病理特征。方法: 回顾性收集2010年1月至2023年9月北京大学第三医院收治的行根治性肾切除术或者保留肾单位手术且术后病理明确为具有低度恶性潜能的多房囊性肾肿瘤患者的临床资料,获取其基本临床特征、术后病理结果及预后。根据手术方式将患者分为根治性肾切除术组及保留肾单位手术组,并比较两组患者的临床病理特征差异。结果: 共纳入35例患者,诊断时的中位年龄为53.0(39.0~62.0)岁,其中23例为男性(65.7%),12例为女性(34.3%)。9例患者接受了根治性肾切除术(25.7%),26例患者接受了保留肾单位手术(74.3%)。35例患者的临床T分期均未超过T2a期。中位手术时间145.0 min,中位估计术中出血量20.0 mL。术后中位住院天数6.0 d。术后病理结果均未提示肾窦侵犯、肉瘤样变、肾上腺侵犯及淋巴结侵犯。将患者根据手术方式分为保留肾单位手术组和根治性肾切除术组,并对两组的临床病理特征进行对比,差异均无统计学意义。除1例患者失访外,其余患者均获随访,随访时间8~111个月,中位随访时间70.5个月,仅1例患者因非肿瘤原因死亡,其余患者均无肿瘤转移或复发。结论: 具有低度恶性潜能的多房囊性肾肿瘤患者的预后较好; 对于具有低度恶性潜能的多房囊性肾肿瘤,接受保留肾单位手术和根治性肾切除术的患者临床病理学特征差异无统计学意义。
中图分类号:
- R737.1

| 1 |
Siegel RL , Miller KD , Fuchs HE , et al. Cancer statistics, 2022[J]. CA Cancer J Clin, 2022, 72 (1): 7- 33.
doi: 10.3322/caac.21708 |
| 2 |
Moch H , Cubilla AL , Humphrey PA , et al. The 2016 WHO classification of tumours of the urinary system and male genital organs. Part A: Renal, penile, and testicular tumours[J]. Eur Urol, 2016, 70 (1): 93- 105.
doi: 10.1016/j.eururo.2016.02.029 |
| 3 |
Li T , Chen J , Jiang Y , et al. Multilocular cystic renal cell neoplasm of low malignant potential: A series of 76 cases[J]. Clin Genitourin Cancer, 2016, 14 (6): e553- e557.
doi: 10.1016/j.clgc.2016.03.017 |
| 4 |
Westerman ME , Cheville JC , Lohse CM , et al. Long-term outcomes of patients with low grade cystic renal epithelial neoplasms[J]. Urology, 2019, 133, 145- 150.
doi: 10.1016/j.urology.2019.07.017 |
| 5 |
Suzigan S , López-Beltrán A , Montironi R , et al. Multilocular cystic renal cell carcinoma: A report of 45 cases of a kidney tumor of low malignant potential[J]. Am J Clin Pathol, 2006, 125 (2): 217- 222.
doi: 10.1309/AH6FC77PYR2V6YAY |
| 6 |
Kashan M , Ghanaat M , Hötker AM , et al. Cystic renal cell carcinoma: A report on outcomes of surgery and active surveillance in patients retrospectively identified on pretreatment imaging[J]. J Urol, 2018, 200 (2): 275- 282.
doi: 10.1016/j.juro.2018.02.3087 |
| 7 |
Silverman SG , Pedrosa I , Ellis JH , et al. Bosniak classification of cystic renal masses, version 2019: An update proposal and needs assessment[J]. Radiology, 2019, 292 (2): 475- 488.
doi: 10.1148/radiol.2019182646 |
| 8 |
Alrumayyan M , Raveendran L , Lawson KA , et al. Cystic renal masses: Old and new paradigms[J]. Urol Clin North Am, 2023, 50 (2): 227- 238.
doi: 10.1016/j.ucl.2023.01.003 |
| 9 |
Yang B , Sun L , Cao WF , et al. Clear cell renal cell carcinoma with cystic component similar to multilocular cystic renal neoplasm of low malignant potential: A rare pattern of cyst-dependent progression from multilocular cystic renal neoplasm of low malignant potential[J]. Diagn Pathol, 2023, 18 (1): 27.
doi: 10.1186/s13000-023-01315-x |
| 10 |
Pini GM , Lucianò R , Colecchia M . Cystic clear cell renal cell carcinoma: A morphological and molecular reappraisal[J]. Can-cers (Basel), 2023, 15 (13): 3352.
doi: 10.3390/cancers15133352 |
| 11 |
Kim SH , Park WS , Chung J . SETD2, GIGYF2, FGFR3, BCR, KMT2C, and TSC2 as candidate genes for differentiating multi-locular cystic renal neoplasm of low malignant potential from clear cell renal cell carcinoma with cystic change[J]. Investig Clin Urol, 2019, 60 (3): 148- 155.
doi: 10.4111/icu.2019.60.3.148 |
| 12 |
Raspollini MR , Castiglione F , Martignoni G , et al. Unlike in clear cell renal cell carcinoma, KRAS is not mutated in multilocular cystic clear cell renal cell neoplasm of low potential[J]. Virchows Arch, 2015, 467 (6): 687- 693.
doi: 10.1007/s00428-015-1859-8 |
| 13 |
Shan K , Fu A , Liu N , et al. Contrast-enhanced ultrasound (CEUS) vs contrast-enhanced computed tomography for multilocular cystic renal neoplasm of low malignant potential: A retrospective analysis for diagnostic performance study[J]. Medicine (Baltimore), 2020, 99 (46): e23110.
doi: 10.1097/MD.0000000000023110 |
| 14 |
Bhatt JR , Jewett MA , Richard PO , et al. Multilocular cystic renal cell carcinoma: Pathological T staging makes no difference to favorable outcomes and should be reclassified[J]. J Urol, 2016, 196 (5): 1350- 1355.
doi: 10.1016/j.juro.2016.05.118 |
| 15 |
Nassir A , Jollimore J , Gupta R , et al. Multilocular cystic renal cell carcinoma: A series of 12 cases and review of the literature[J]. Urology, 2002, 60 (3): 421- 427.
doi: 10.1016/S0090-4295(02)01742-9 |
| 16 |
Gong K , Zhang N , He Z , et al. Multilocular cystic renal cell carcinoma: An experience of clinical management for 31 cases[J]. J Cancer Res Clin Oncol, 2008, 134 (4): 433- 437.
doi: 10.1007/s00432-007-0302-1 |
| 17 |
Pitra T , Pivovarcikova K , Alaghehbandan R , et al. A comprehensive commentary on the multilocular cystic renal neoplasm of low malignant potential: A urologist' s perspective[J]. Cancers (Basel), 2022, 14 (3): 831.
doi: 10.3390/cancers14030831 |
| 18 |
Cao C , Deng S , Wang B , et al. Intraoperative near-infrared Ⅱ window fluorescence imaging-assisted nephron-sparing surgery for complete resection of cystic renal masses[J]. Clin Transl Med, 2021, 11 (10): e604.
doi: 10.1002/ctm2.604 |
| [1] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [2] | 舒帆, 葛力源, 邓汉彰, 殷昊明, 欧俊永, 邓绍晖, 郝一昌, 陆敏, 张展奕, 段佩辰, 张树栋. 预后不良的肾细胞癌伴淋巴结转移的分子特征[J]. 北京大学学报(医学版), 2026, 58(3): 631-640. |
| [3] | 张铃福, 陈明, 赵小宇, 王港, 崔龙, 凌晓锋, 王立新, 徐智, 郭丽梅, 侯纯升. 原发灶局限于胆囊壁内胆囊癌大体分型及其与预后和癌前病变的相关性[J]. 北京大学学报(医学版), 2026, 58(1): 184-189. |
| [4] | 高雅静, 李正芳, 马梦思, 武丽君. SII和SIRI对白塞病葡萄膜炎的风险预测及疾病活动度和预后的评估[J]. 北京大学学报(医学版), 2025, 57(6): 1067-1073. |
| [5] | 郭博达, 陆敏, 王国良, 张洪宪, 刘磊, 侯小飞, 赵磊, 田晓军, 张树栋. 肾透明细胞癌与非透明细胞癌伴静脉癌栓患者的临床病理特征及预后比较[J]. 北京大学学报(医学版), 2025, 57(4): 644-649. |
| [6] | 刘帅, 刘茁, 管允鹤, 王国良, 田晓军, 张洪宪, 刘磊, 马潞林, 张树栋. 机器人辅助腹腔镜下腔静脉节段性切除术治疗肾肿瘤瘤栓侵犯血管壁[J]. 北京大学学报(医学版), 2025, 57(4): 796-802. |
| [7] | 李伟浩, 李晶, 张学民, 李伟, 李清乐, 张小明. 术中回收式自体输血对颈动脉体瘤切除术后肿瘤预后的影响[J]. 北京大学学报(医学版), 2025, 57(2): 272-276. |
| [8] | 毛雅晴, 陈震, 于尧, 章文博, 刘洋, 彭歆. 2型糖尿病对口腔鳞状细胞癌患者预后的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1089-1096. |
| [9] | 欧俊永,倪坤明,马潞林,王国良,颜野,杨斌,李庚午,宋昊东,陆敏,叶剑飞,张树栋. 肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素[J]. 北京大学学报(医学版), 2024, 56(4): 582-588. |
| [10] | 刘帅,刘磊,刘茁,张帆,马潞林,田晓军,侯小飞,王国良,赵磊,张树栋. 伴静脉癌栓的肾上腺皮质癌的临床治疗及预后[J]. 北京大学学报(医学版), 2024, 56(4): 624-630. |
| [11] | 王滨帅,邱敏,张前进,田茂锋,刘磊,王国良,陆敏,田晓军,张树栋. 6例肾尤文肉瘤伴静脉瘤栓的诊治[J]. 北京大学学报(医学版), 2024, 56(4): 636-639. |
| [12] | 周泽臻,邓绍晖,颜野,张帆,郝一昌,葛力源,张洪宪,王国良,张树栋. 非转移性T3a肾细胞癌患者3年肿瘤特异性生存期预测[J]. 北京大学学报(医学版), 2024, 56(4): 673-679. |
| [13] | 方杨毅,李强,黄志高,陆敏,洪锴,张树栋. 睾丸鞘膜高分化乳头状间皮肿瘤1例[J]. 北京大学学报(医学版), 2024, 56(4): 741-744. |
| [14] | 曾媛媛,谢云,陈道南,王瑞兰. 脓毒症患者发生正常甲状腺性病态综合征的相关因素[J]. 北京大学学报(医学版), 2024, 56(3): 526-532. |
| [15] | 陈克伟,邓绍晖,刘茁,张洪宪,马潞林,张树栋. 肾血管平滑肌脂肪瘤破裂出血的手术时机[J]. 北京大学学报(医学版), 2024, 56(2): 326-331. |
|
||
