北京大学学报(医学版) ›› 2026, Vol. 58 ›› Issue (3): 567-574. doi: 10.19723/j.issn.1671-167X.2026.03.017
围术期高血糖与食管切除术后食管鳞癌不良预后相关性
彭博1,*, 刘芳芳1,*, 杨伟2, 徐瑞平3, 陈蕾2, 李保中3, 王新家2, 柯骥1, 杨文蕾1, 何煜4, 刘震1, 侯波林5, 张利群2, 林妙萍2, 张立新3, 张凡2, 蔡奋2, 许铧文2, 刘萌飞1, 刘英1, 潘雅琪1, 何忠虎6,*( ), 柯杨6,*()
), 柯杨6,*()
- 1. 北京大学肿瘤医院暨北京市肿瘤防治研究所遗传学研究室,恶性肿瘤发病机制及转化研究教育部重点实验室,北京 100142
2. 汕头大学医学院附属肿瘤医院,广东汕头 515031
3. 安阳市肿瘤医院, 河南安阳 455000
4. 中华预防医学会, 北京 100062
5. 零氪科技(北京)有限公司,北京 100080
6. 北京大学肿瘤医院暨北京市肿瘤防治研究所遗传学研究室,分子肿瘤学全国重点实验室,北京 100142
Perioperative hyperglycemia predicts poorer prognosis of esophageal squamous cell carcinoma patients treated with esophagectomy
Bo PENG1, Fangfang LIU1, Wei YANG2, Ruiping XU3, Lei CHEN2, Baozhong LI3, Xinjia WANG2, Ji KE1, Wenlei YANG1, Yu HE4, Zhen LIU1, Bolin HOU5, Liqun ZHANG2, Miaoping LIN2, Lixin ZHANG3, Fan ZHANG2, Fen CAI2, Huawen XU2, Mengfei LIU1, Ying LIU1, Yaqi PAN1, Zhonghu HE6,*(), Yang KE6,*()
- 1. Key Laboratory of Carcinogenesis and Translational Research(Ministry of Education), Department of Genetics, Peking University Cancer Hospital & Institute, Beijing 100142, China
2. Cancer Hospital of Shantou University Medical College, Shantou 515031, Guangdong, China
3. Anyang Cancer Hospital, Anyang 455000, Henan, China
4. Chinese Preventive Medicine Association, Beijing 100062, China
5. Linkdoc AI Research(LAIR), Beijing 100080, China
6. State Key Laboratory of Molecular Oncology, Department of Genetics, Peking University Cancer Hospital & Institute, Beijing 100142, China
摘要:
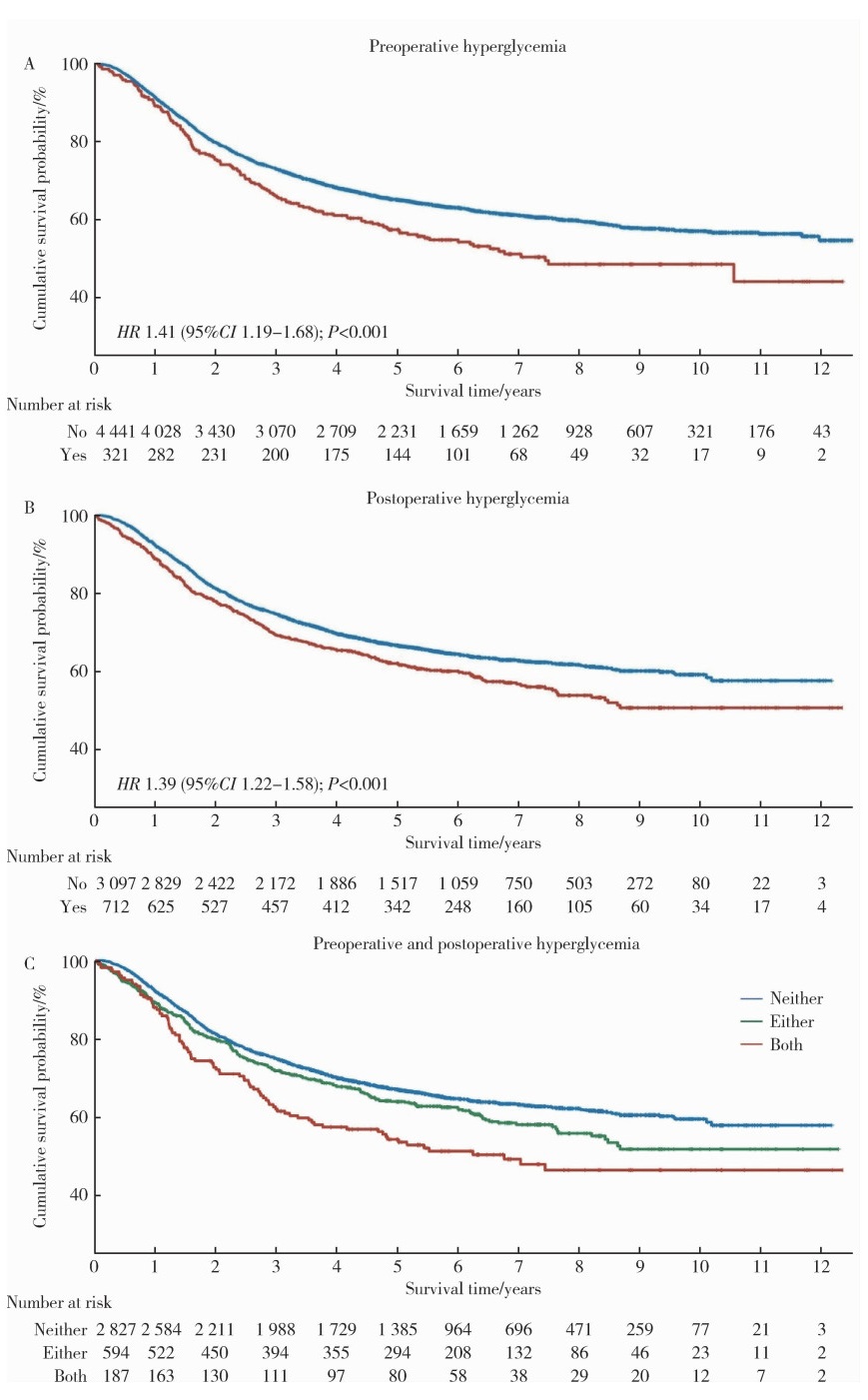
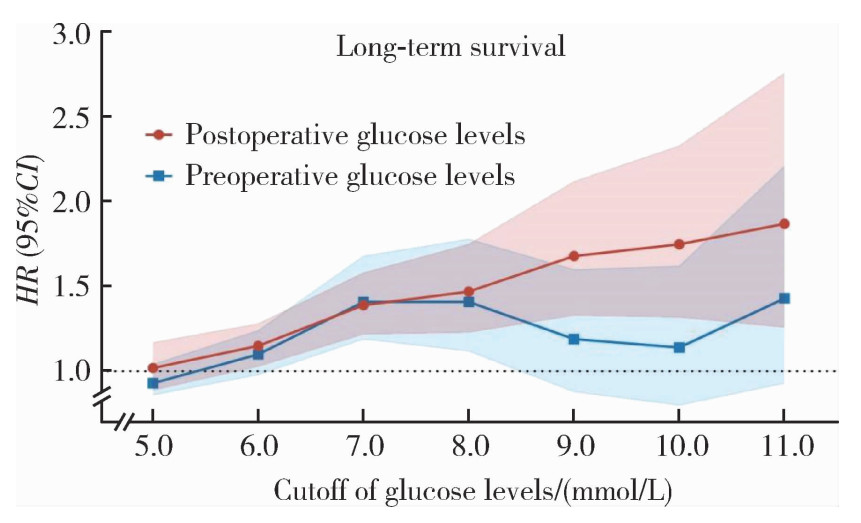
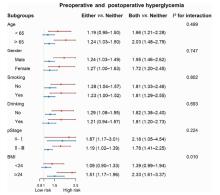
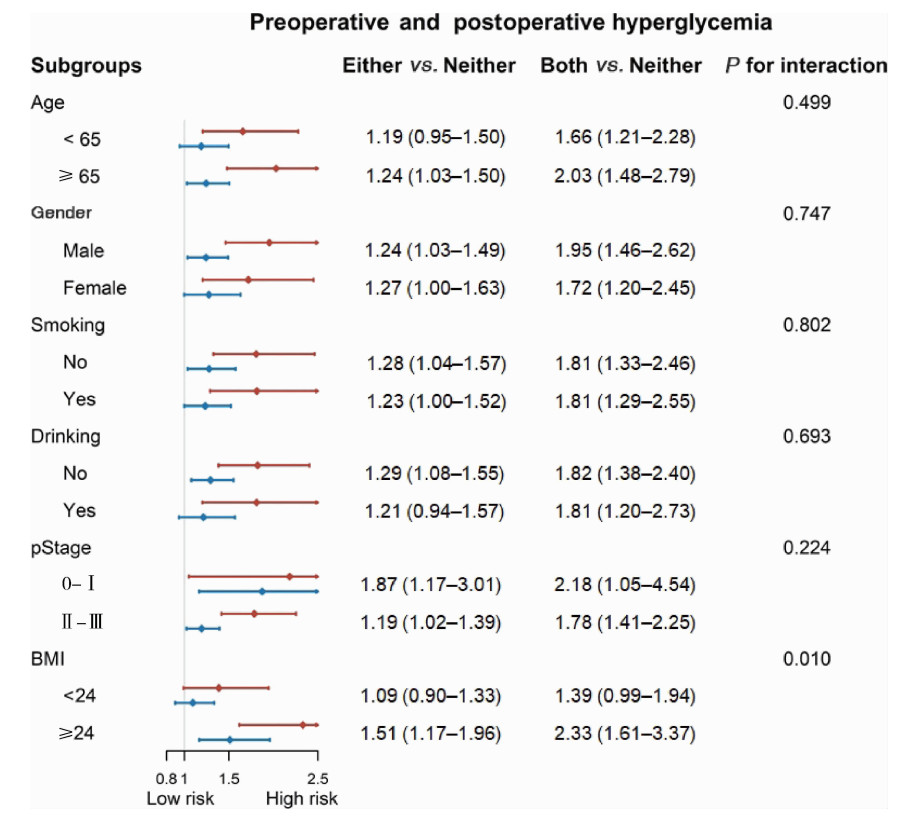
目的: 基于大样本、多中心真实世界数据,系统评估围术期高血糖与食管鳞癌(esophageal squamous cell carcinoma,ESCC)患者术后预后之间的关联。方法: 连续纳入河南省安阳市肿瘤医院(2012年1月至2017年12月)与广东省汕头大学医学院附属肿瘤医院(2009年8月至2018年12月)接受根治性食管切除术的5 952例ESCC患者的病例资料进行回顾性队列研究,围术期空腹血糖数据来源于医院信息系统。将围术期划分为术前和术后两个阶段,术前高血糖定义为术前第14天至第2天平均空腹血糖≥7.0 mmol/L,术后高血糖定义为术后第2天至第14天平均空腹血糖≥7.0 mmol/L。主要结局为总生存期,次要结局包括术后30 d/90 d死亡率及住院期间并发症。采用多因素Cox比例风险模型,评估围术期高血糖与总生存的关联,计算校正后的风险比(hazard ratio,HR)及其95%置信区间(confidence interval,CI)。结果: 研究人群最长随访时间达12年。术前与术后高血糖发生率分别为6.7%和18.3%。术前高血糖患者的5年总生存率低于非高血糖患者(57.3% vs. 65.0%),校正后HR为1.41(95%CI:1.19~1.68);术后高血糖患者的5年生存率亦较低(61.8% vs. 66.4%),校正后HR为1.39(95%CI:1.22~1.58)。联合分析显示,与无高血糖者相比,仅在术前或术后单一阶段出现高血糖的患者死亡风险升高(HR=1.24,95%CI:1.07~1.43),而术前和术后均存在高血糖的患者死亡风险最高(HR=1.86,95% CI:1.49~2.32)。分层分析显示,体重指数(body mass index,BMI)显著修饰了高血糖与不良预后的关联(交互作用P=0.010),该关联在BMI≥24.0 kg/m2的患者中尤为显著。此外,围术期高血糖亦与较差的术后短期结局相关。结论: 围术期高血糖是接受根治性食管切除术的ESCC患者术后长期生存的独立危险因素,提示在ESCC围术期管理过程中加强常规血糖监测与控制,可能有助于改善患者的长期预后。
中图分类号:
- R735.1

| 1 |
|
| 2 |
doi: 10.1136/gutjnl-2014-308124 |
| 3 |
doi: 10.1053/j.gastro.2017.08.023 |
| 4 |
doi: 10.20892/j.issn.2095-3941.2016.0093 |
| 5 |
doi: 10.1093/dote/doz091 |
| 6 |
doi: 10.1111/j.1442-2050.2008.00901.x |
| 7 |
doi: 10.1007/s10388-022-00950-5 |
| 8 |
|
| 9 |
doi: 10.1152/physrev.00030.2014 |
| 10 |
|
| 11 |
doi: 10.1097/SLA.0b013e31820b4bfc |
| 12 |
doi: 10.1097/00000658-200005000-00003 |
| 13 |
doi: 10.1186/s40880-018-0275-2 |
| 14 |
doi: 10.1093/dote/doz098 |
| 15 |
doi: 10.1016/j.ebiom.2017.01.035 |
| 16 |
doi: 10.1016/j.annepidem.2016.11.004 |
| 17 |
doi: 10.1016/j.eclinm.2020.100312 |
| 18 |
doi: 10.1245/s10434-010-1024-1 |
| 19 |
|
| 20 |
doi: 10.1503/cmaj.110977 |
| 21 |
doi: 10.1161/01.STR.0000085087.41330.FF |
| 22 |
doi: 10.1161/01.CIR.36.4.609 |
| 23 |
doi: 10.1093/qjmed/hcu218 |
| 24 |
|
| [1] | 袁思妍, 闵鹤葳, 陈平, 吴一波, 崔红霞, 张旭熙, 孙昕霙. 基于大五人格特质的2型糖尿病患者健康教育偏好[J]. 北京大学学报(医学版), 2026, 58(3): 600-605. |
| [2] | 舒帆, 葛力源, 邓汉彰, 殷昊明, 欧俊永, 邓绍晖, 郝一昌, 陆敏, 张展奕, 段佩辰, 张树栋. 预后不良的肾细胞癌伴淋巴结转移的分子特征[J]. 北京大学学报(医学版), 2026, 58(3): 631-640. |
| [3] | 张铃福, 陈明, 赵小宇, 王港, 崔龙, 凌晓锋, 王立新, 徐智, 郭丽梅, 侯纯升. 原发灶局限于胆囊壁内胆囊癌大体分型及其与预后和癌前病变的相关性[J]. 北京大学学报(医学版), 2026, 58(1): 184-189. |
| [4] | 田雪丽, 宋志强, 黄永辉, 姚炜. 肌萎缩侧索硬化患者经皮内镜下胃造瘘术后早期并发症及相关危险因素分析[J]. 北京大学学报(医学版), 2026, 58(1): 190-195. |
| [5] | 高雅静, 李正芳, 马梦思, 武丽君. SII和SIRI对白塞病葡萄膜炎的风险预测及疾病活动度和预后的评估[J]. 北京大学学报(医学版), 2025, 57(6): 1067-1073. |
| [6] | 王晓林, 郭邵逸, 陈大召, 温锡杰, 华勇, 张亮, 张秦. 全髋关节置换术治疗系统性红斑狼疮继发股骨头缺血性坏死的随访研究[J]. 北京大学学报(医学版), 2025, 57(6): 1081-1088. |
| [7] | 闵鹤葳, 吴一波, 史宇晖, 李明子, 孙昕霙. 基于健康行动过程取向模型分析2型糖尿病患者膳食模式及血糖控制的影响因素[J]. 北京大学学报(医学版), 2025, 57(6): 1145-1152. |
| [8] | 顾静妍, 李欣艺, 赵金霞, 穆荣. 误诊为类风湿关节炎、痛风的糖尿病致Charcot关节病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1193-1197. |
| [9] | 曹沛, 栾庆先. 牙周炎与全身系统性疾病的思考与探索[J]. 北京大学学报(医学版), 2025, 57(5): 852-858. |
| [10] | 郭博达, 陆敏, 王国良, 张洪宪, 刘磊, 侯小飞, 赵磊, 田晓军, 张树栋. 肾透明细胞癌与非透明细胞癌伴静脉癌栓患者的临床病理特征及预后比较[J]. 北京大学学报(医学版), 2025, 57(4): 644-649. |
| [11] | 左超, 王国立, 杨昆霖, 车新艳, 孟一森, 张凯. 前列腺体积不同的患者经尿道光纤铥激光前列腺剜除术的有效性及安全性比较[J]. 北京大学学报(医学版), 2025, 57(4): 711-716. |
| [12] | 赵兆, 张维宇, 杨文博, 张勇杰, 张晓鹏, 赵慧颖, 周刚, 王强. 低龄、低体重儿童肾移植2例[J]. 北京大学学报(医学版), 2025, 57(4): 803-807. |
| [13] | 陈子砚, 张晓悦, 顾亦梧, 常春. 2型糖尿病患者使用E-health管理疾病意愿与影响机制[J]. 北京大学学报(医学版), 2025, 57(3): 522-528. |
| [14] | 李伟浩, 李晶, 张学民, 李伟, 李清乐, 张小明. 术中回收式自体输血对颈动脉体瘤切除术后肿瘤预后的影响[J]. 北京大学学报(医学版), 2025, 57(2): 272-276. |
| [15] | 王菲, 张馨月, 刘木清, 王恩博, 段登辉. 顺牙长轴拔牙法在下颌近中与水平智齿拔除术中的应用及三维有限元分析[J]. 北京大学学报(医学版), 2025, 57(1): 106-112. |
|
||
