北京大学学报(医学版) ›› 2018, Vol. 50 ›› Issue (6): 1098-1101. doi: 10.19723/j.issn.1671-167X.2018.06.028
盆腹腔软组织侵袭性血管黏液瘤临床病理分析
刘蕾( ),王丽华,任玉波,饶晓松,杨邵敏
),王丽华,任玉波,饶晓松,杨邵敏
- 北京大学国际医院病理科, 北京 102206
Clinicopathological analysis of aggressive angiomyxoma of soft tissue in abdomino-pelvic cavity
Lei LIU(),Li-hua WANG,Yu-bo REN,Xiao-song RAO,Shao-min YANG
- Department of Pathology, Peking University International Hospital, Beijing 102206, China
摘要:
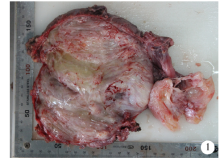
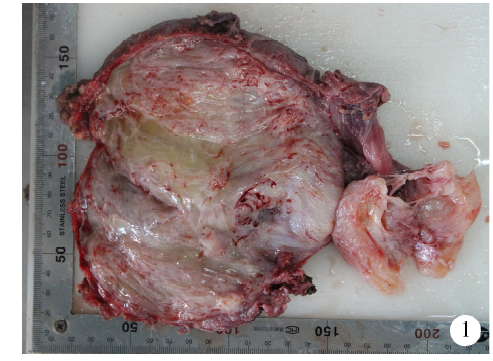
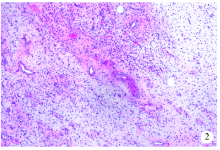
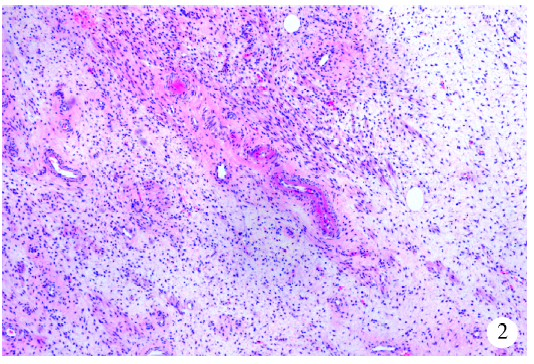
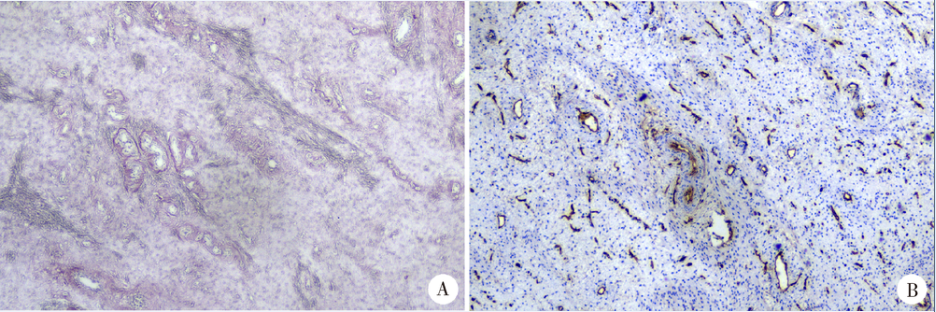
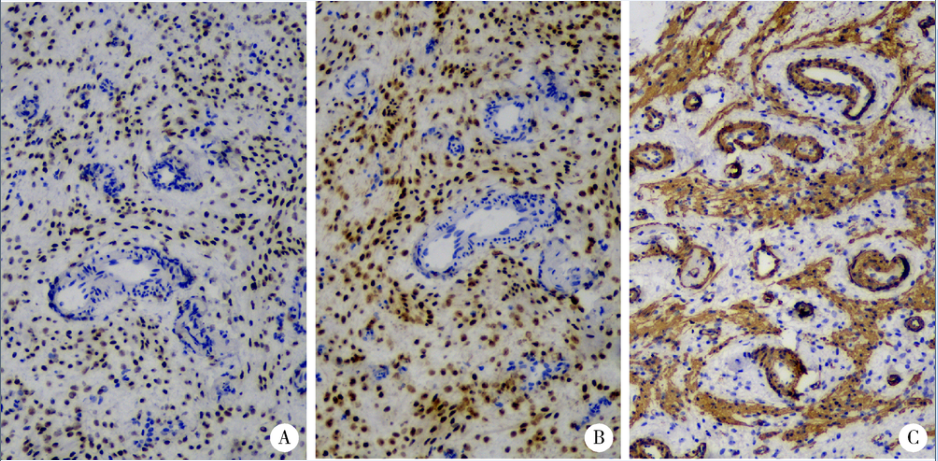
侵袭性血管黏液瘤是一种少见的间叶性肿瘤,为探讨其临床病理学特征、诊治及预后,本研究收集北京大学国际医院4例盆腹腔软组织侵袭性血管黏液瘤的临床影像资料,分析其病理学形态、免疫表型及治疗随访情况,并回顾相关文献。本组4例均为女性,年龄27~49岁,平均年龄33岁,无诱因腹胀或无明显不适经体检发现,3例原发、1例复发。3例CT及磁共振扫描可见分层/漩涡征。肿瘤主体均位于盆腔,1例同时累及腹腔。肿瘤最大径5~22 cm,切面灰白、灰黄色,实性,质软,灶性水肿或囊性改变。显微镜下瘤细胞短梭形,异型不明显,间质富疏松水肿黏液或胶原,有丰富的薄壁及厚壁血管,部分血管壁玻璃样变性。肿瘤可浸润周围脂肪、神经组织。免疫组织化学染色提示4例肿瘤均雌激素受体、孕激素受体、结蛋白、平滑肌肌动蛋白弥漫阳性,CD34仅血管表达,S-100蛋白、CD117、Dog1均阴性。手术完整切除肿瘤,术后随访有1例二次复发。侵袭性血管黏液瘤确诊以病理形态学为基础,辅以免疫组织化学进一步诊断及鉴别诊断;手术切除后可多次复发。
中图分类号:
- R739.9

| [1] | Fletcher CDM, Bridge JA, Hogendoorn PCW , et al. World Health Organization classification of tumours of soft tissue and bone [M]. Lyon: IARC Press, 2013. |
| [2] |
Zhang JP, Zhu CF . Clinical experiences on aggressive angio-myxoma in China (report of 93 cases)[J]. Int J Gynecol Cancer, 2010,20(2):303-307.
doi: 10.1111/IGC.0b013e3181cc339c pmid: 20134274 |
| [3] |
Ahmed MA, Uehelie MA, Rage AM , et al. Aggressive angio-myxoma of the penis: the first case report in a 9-month-old infant[J]. Urology, 2017,104(6):187-190.
doi: 10.1016/j.urology.2016.12.045 |
| [4] |
Surabhi VR, Garg N, Frumovitz M , et al. Aggressive angio-myxomas: a comprehensive imaging review with clinical and histopathologic correlation[J]. Am J Roentgenol, 2014,202(6):1171-1178.
doi: 10.2214/AJR.13.11668 pmid: 24848813 |
| [5] |
Petscavage-Thomas JM, Walker EA, Logie CI , et al. Soft-tissue myxomatous lesions: review of salient imaging features with pathologic comparison[J]. Radiographics, 2014,34(4):964-980.
doi: 10.1148/rg.344130110 pmid: 25019435 |
| [6] |
Sun Y, Zhu L, Chang X , et al. Clinicopathological features and treatment analysis of rare aggressive angiomyxoma of the female pelvis and perineum: a retrospective study[J]. Pathol Oncol Res, 2017,23(1):131-137.
doi: 10.1007/s12253-016-0109-y pmid: 27571990 |
| [7] |
Chen H, Zhao H, Xie Y , et al. Clinicopathological features and differential diagnosis of aggressive angiomyxoma of the female pelvis: 5 case reports and literature review[J]. Medicine (Baltimore), 2017,96(20):e6820.
doi: 10.1097/MD.0000000000006820 |
| [8] |
魏红权, 刘珺, 冯晶晶 . 侵袭性血管黏液瘤临床病理观察[J]. 中华医学杂志, 2012,92(22):1553-1555.
doi: 10.3760/cma.j.issn.0376-2491.2012.22.013 |
| [9] |
Alameda F, Munne A, Baro T , et al. Vulvar angiomyxoma, aggressive angiomyxoma, and angiomyofibroblastoma: an immunohistochemical and ultrastructural study[J]. Ultrastruct Pathol, 2006,30(3):193-205.
doi: 10.1080/01913120500520911 pmid: 16825121 |
| [10] |
Rawlinson NJ, West WW, Nelson M , et al. Aggressive angio-myxoma with t(12;21) and HMGA2 rearrangement: report of a case and review of the literature[J]. Cancer Genet Cytogenet, 2008,181(2):119-124.
doi: 10.1016/j.cancergencyto.2007.11.008 pmid: 18295664 |
| [11] |
Jiang XX, Qian LH, Xu HK , et al. Mutation of an X chromosome in aggressive angiomyxoma: Report of a case and review of the literature[J]. Gynecol Oncol Case Rep, 2011,2(2):39-41.
doi: 10.1016/j.gynor.2011.12.001 pmid: 3860615 |
| [12] |
Bai HM, Yang JX, Huang HF , et al. Individualized managing strategies of aggressive angiomyxoma of female genital tract and pelvis[J]. Eur J Surg Oncol, 2013,39(10):1101-1108.
doi: 10.1016/j.ejso.2013.06.013 pmid: 23899874 |
| [13] |
Han-Geurts IJ, van Geel AN, van Doorn L , et al. Aggressive angiomyxoma: multimodality treatments can avoid mutilating surgery[J]. Eur J Surg Oncol, 2006,32(10):1217-1221.
doi: 10.1016/j.ejso.2006.06.008 pmid: 16870390 |
| [14] |
Orfanelli T, Kim CS, Vitez SF , et al. A case report of aggressive angiomyxoma in pregnancy: do hormones play a role[J]. Case Rep Obstet Gynecol, 2016(3):1-4.
doi: 10.1155/2016/6810368 |
| [15] |
宫丽华, 孙晓淇, 孟淑琴 , 等. 骨内侵袭性血管黏液瘤的诊断及与其他黏液性骨肿瘤的鉴别[J]. 临床与实验病理学杂志, 2012,28(10):1143-1145.
doi: 10.3969/j.issn.1001-7399.2012.10.019 |
| [16] |
Schwartz PE, Hui P , McCarthy S. Hormonal therapy for aggressive angiomyxoma: a case report and proposed management algorithm[J]. J Low Genit Tract Dis, 2014,18(2):55-61.
doi: 10.1097/LGT.0b013e3182a22019 |
| [17] |
Wang Z, Liu Y, Yang L , et al. Maxillary aggressive angiomyxoma showing ineffective to radiotherapy: a rare case report and review of literature[J]. Int J Clin Exp Pathol, 2015,8(1):1063-1067.
pmid: 25755820 |
| [18] |
Coppola S, Desai A, Tzanis D , et al. Conservative en bloc surgery for aggressive angiomyxoma achieves good local control: analysis of 14 patients from a single institution[J]. Int J Gynecol Cancer, 2013,23(3):540-545.
doi: 10.1097/IGC.0b013e3182843063 |
| [19] |
Blandamura S, Cruz J, Faure Vergara L , et al. Aggressive angiomyxoma: a second case of metastasis with patient’s death[J]. Hum Pathol, 2003,34(10):1072-1074.
doi: 10.1053/S0046-8177(03)00419-2 pmid: 14608546 |
| [20] |
Geng J, Cao B, Wang L . Aggressive angiomyxoma: an unusual presentation[J]. Korean J Radiol, 2012,13(1):90-93.
doi: 10.3348/kjr.2012.13.1.90 pmid: 22247641 |
| [1] | 赵业, 刁小莉, 熊焰. 细胞转移技术在微量细胞液病理诊断中的应用[J]. 北京大学学报(医学版), 2026, 58(1): 208-213. |
| [2] | 王晓林, 李璐瑶, 张雯, 王鸿雁. 3例子宫体中肾样腺癌的临床病理学分析[J]. 北京大学学报(医学版), 2025, 57(6): 1208-1212. |
| [3] | 王小梦, 曾晓君, 李娟. 黎族与汉族系统性红斑狼疮患者的主要临床特征[J]. 北京大学学报(医学版), 2025, 57(6): 1213-1218. |
| [4] | 张展奕, 陆敏, 孙悦皓, 董靖晗, 侯小飞, 肖春雷, 王国良, 田晓军, 马潞林, 张洪宪, 张树栋. TFE3重排肾细胞癌合并静脉癌栓患者的临床病理特征及生存分析[J]. 北京大学学报(医学版), 2025, 57(4): 650-661. |
| [5] | 孙建军, 马千权, 尹晓亮, 杨辰龙, 张嘉, 陈素华, 吴超, 谢京城, 韩芸峰, 林国中, 司雨, 杨军, 邬海博, 赵强. 任意维度重建磁共振对骶管囊肿进行精准分型对于指导微创手术和康复的意义[J]. 北京大学学报(医学版), 2025, 57(2): 303-308. |
| [6] | 王红彦, 李鑫铭, 房柯池, 朱华群, 贾汝琳, 王晶. 系统性红斑狼疮疾病活动度相关特征分析及评估模型的构建[J]. 北京大学学报(医学版), 2024, 56(6): 1017-1022. |
| [7] | 罗丹, 黄海建, 陈新, 陈小岩. 原发子宫肝样腺癌2例临床病理分析及文献复习[J]. 北京大学学报(医学版), 2024, 56(6): 1126-1131. |
| [8] | 赵亮, 史成龙, 马柯, 赵静, 王潇, 邢晓燕, 莫万星, 练益瑞, 高超, 李玉慧. 抗合成酶综合征重叠类风湿关节炎患者的免疫学特征[J]. 北京大学学报(医学版), 2024, 56(6): 972-979. |
| [9] | 邢念增,王明帅,杨飞亚,尹路,韩苏军. 前列腺免活检创新理念的临床实践及其应用前景[J]. 北京大学学报(医学版), 2024, 56(4): 565-566. |
| [10] | 田宇轩,阮明健,刘毅,李德润,吴静云,沈棋,范宇,金杰. 双参数MRI改良PI-RADS评分4分和5分病灶的最大径对临床有意义前列腺癌的预测效果[J]. 北京大学学报(医学版), 2024, 56(4): 567-574. |
| [11] | 刘帅,刘磊,刘茁,张帆,马潞林,田晓军,侯小飞,王国良,赵磊,张树栋. 伴静脉癌栓的肾上腺皮质癌的临床治疗及预后[J]. 北京大学学报(医学版), 2024, 56(4): 624-630. |
| [12] | 赖展鸿,李嘉辰,贠泽霖,张永刚,张昊,邢晓燕,邵苗,金月波,王乃迪,李依敏,李玉慧,栗占国. 特发性炎性肌病完全临床应答相关因素的单中心真实世界研究[J]. 北京大学学报(医学版), 2024, 56(2): 284-292. |
| [13] | 徐训敏,邵校,姬爱平. 口腔急诊科死亡病例分析[J]. 北京大学学报(医学版), 2024, 56(1): 185-189. |
| [14] | 冯璐,翟佳羽,赵金霞. IgG4相关性疾病患者就诊情况及其临床特征[J]. 北京大学学报(医学版), 2023, 55(6): 1028-1032. |
| [15] | 薛子璇,唐世英,邱敏,刘承,田晓军,陆敏,董靖晗,马潞林,张树栋. 青年肾肿瘤伴瘤栓的临床病理特征及预后分析[J]. 北京大学学报(医学版), 2023, 55(5): 802-811. |
|
||
