北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (4): 614-620. doi: 10.19723/j.issn.1671-167X.2020.04.003
血浆游离型甲氧基肾上腺素类物质检测正常的嗜铬细胞瘤和副神经节瘤的临床特点
刘鹭1,田杰2,吴恺1,高莹1,△( ),张争2,△(),张俊清1,郭晓蕙1
),张争2,△(),张俊清1,郭晓蕙1
- 1.北京大学第一医院 内分泌科,北京 100034
2.北京大学第一医院 内分泌科泌尿外科,北京 100034
Clinical profile of pheochromocytoma and paraganglioma with normal plasma free metanephrines
Lu LIU1,Jie TIAN2,Kai WU1,Ying GAO1,△(),Zheng ZHANG2,△(),Jun-qing ZHANG1,Xiao-hui GUO1
- 1. Department of Endocrinology, Peking University First Hospital, Beijing 100034, China
2. Department of Urology, Peking University First Hospital, Beijing 100034, China
摘要:
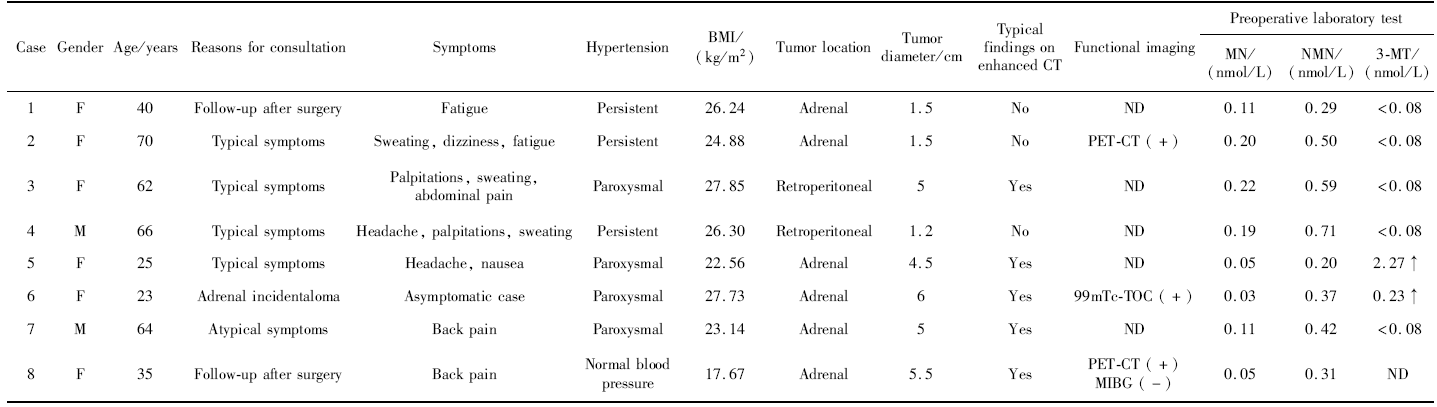
目的: 分析散发嗜铬细胞瘤和副神经节瘤(pheochromocytoma and paraganglioma,PPGL)患者中血浆游离型甲氧基肾上腺素类物质(metanephrines,MNs)正常者的临床特点,MNs已作为PPGL的首选检测方法在临床中广泛应用,MNs正常的PPGL较少见。方法: 选择2015年3月—2020年1月于北京大学第一医院行泌尿外科手术,病理确诊为PPGL的散发患者共104例,所有患者均有术前血浆游离型MNs检测结果,其中8例(7.69%)MNs正常。回顾MNs正常患者的就诊原因,临床表现,术前检测血浆游离型MNs、3-甲氧基酪胺(3-methoxytyramine, 3-MT)、血儿茶酚胺和嗜铬粒蛋白A(chromograninA, CgA)的结果,影像学表现,术前诊断,术前用药准备,术中血压波动情况及肿瘤组织病理学特点,并与同期MNs升高的PPGL患者相比较。对MNs正常患者进行术后随访。结果: MNs正常的8例PPGL患者中,最常见的临床症状为多汗(3/8)、腰腹痛(3/8)、头痛(2/8)、心悸(2/8)和疲乏(2/8)。对比MNs正常组和升高组患者的其他生化检验结果,血3-MT、儿茶酚胺诊断阳性率组间差异无统计学意义,血浆CgA诊断阳性率在MNs正常组显著下降(2/5 vs.41/43,P=0.005)。两组患者增强CT出现典型表现的比例差异无统计学意义。在8例MNs正常患者中,6例因明确的PPGL既往史,或典型的症状及CT表现,3-MT、CgA升高,PET-CT阳性等原因诊断为PPGL,2例误诊为无功能腺瘤或原发性醛固酮增多症。全部MNs正常患者均应用α受体阻滞剂术前准备,其中1例出现术中平均动脉压<60 mmHg。8例术后随访的中位时间为1.5(0.5~4.5)年,增强CT检查均未见新发肿瘤证据。2例MNs正常患者术后复查3-MT和(或)CgA降至正常。结论: 对于出现PPGL典型症状的肾上腺或腹膜后肿瘤患者及有PPGL既往史患者,MNs检测正常不能作为排除PPGL的充分依据。血3-MT、儿茶酚胺、CgA及影像学检查或对PPGL的诊断有帮助。怀疑MNs正常的PPGL患者推荐应用α受体阻滞剂术前准备,但应避免过量。MNs正常患者的术后随访应重点监测术前阳性的生化指标。
中图分类号:
- R736

| [1] |
Lenders JW, Pacak K, Walther MM, et al. Biochemical diagnosis of pheochromocytoma: which test is best[J]. JAMA, 2002,287(11):1427-1434.
doi: 10.1001/jama.287.11.1427 pmid: 11903030 |
| [2] |
Unger N, Pitt C, Schmidt IL, et al. Diagnostic value of various biochemical parameters for the diagnosis of pheochromocytoma in patients with adrenal mass[J]. Eur J Endocrinol, 2006,154(3):409-417.
pmid: 16498054 |
| [3] | Hickman PE, Leong M, Chang J, et al. Plasma free metanephrines are superior to urine and plasma catecholamines and urine catecholamine metabolites for the investigation of phaeochromocytoma[J]. Pathology, 2009,41(2):173-177. |
| [4] |
Grouzmann E, Drouard-Troalen L, Baudin E, et al. Diagnostic accuracy of free and total metanephrines in plasma and fractionated metanephrines in urine of patients with pheochromocytoma[J]. Eur J Endocrinol, 2010,162(5):951-960.
pmid: 20142367 |
| [5] |
Unger N, Hinrichs J, Deutschbein T, et al. Plasma and urinary metanephrines determined by an enzyme immunoassay, but not serum chromogranin A for the diagnosis of pheochromocytoma in patients with adrenal mass[J]. Exp Clin Endocrinol Diabetes, 2012,120(8):494-500.
doi: 10.1055/s-0032-1309007 pmid: 22696168 |
| [6] | Lenders JW, Duh QY, Eisenhofer G, et al. Pheochromocytoma and paraganglioma: an endocrine society clinical practice guideline[J]. J Clin Endocrinol Metab, 2014,99(6):1915-1942. |
| [7] | 中华医学会内分泌学分会肾上腺学组. 嗜铬细胞瘤和副神经节瘤诊断治疗的专家共识[J]. 中华内分泌代谢杂志, 2016,32(3):181-187. |
| [8] | Plouin PF, Amar L, Dekkers OM, et al. European society of endocrinology clinical practice guideline for long-term follow-up of patients operated on for a phaeochromocytoma or a paraganglioma[J]. Eur J Endocrinol, 2016,174(5):G1-G10. |
| [9] |
Bozin M, Lamb A, Putra LJ. Pheochromocytoma with negative metanephrines: a rarity and the significance of dopamine secreting tumors[J]. Urol Case Rep, 2017,12:51-53.
pmid: 28337414 |
| [10] | 曹万里, 黄宝星, 成康, 等. 血浆游离甲氧肾上腺素和甲氧基去甲肾上腺素正常的嗜铬细胞瘤/副神经节瘤患者的临床特点[J]. 中华临床医师杂志: 电子版, 2015,9(2):200-205. |
| [11] | 刘颖姝, 李乐乐, 窦京涛, 等. 偶发嗜铬细胞瘤患者术中血流动力学变化的相关因素[J]. 中华医学杂志, 2018,98(36):2905-2909. |
| [12] | Poudyal S, Pradhan M, Chapagain S, et al. Marker-negative pheochromocytoma associated with inferior vena cava thrombosis[J/OL]. Case Rep Urol, 2017, 2017: 6270436(2017-06-15)[2020-03-01]. https://www.hindawi.com/journals/criu/2017/6270436/. |
| [13] |
Lopez-Gomez J, Salazar-Alvarez MA, Adame RY, et al. Metasta-tic pheochromocytoma to liver without elevation of metanephrines and catecholamines[J]. Int J Surg Case Rep, 2016,29:71-75.
pmid: 27821293 |
| [14] | Kota SK, Kota SK, Panda S, et al. Pheochromocytoma: an uncommon presentation of an asymptomatic and biochemically silent adrenal incidentaloma[J]. Malays J Med Sci, 2012,19(2):86-91. |
| [15] |
Heavner MG, Krane LS, Winters SM, et al. Pheochromocytoma diagnosed pathologically with previous negative serum markers[J]. J Surg Oncol, 2015,112(5):492-495.
pmid: 26384104 |
| [16] |
Eisenhofer G, Lenders JW, Goldstein DS, et al. Pheochromocytoma catecholamine phenotypes and prediction of tumor size and location by use of plasma free metanephrines[J]. Clin Chem, 2005,51(4):735-744.
pmid: 15718487 |
| [17] |
Pillai D, Ross HA, Kratzsch J, et al. Proficiency test of plasma free and total metanephrines: report from a study group[J]. Clin Chem Lab Med, 2009,47(6):786-790.
pmid: 19445649 |
| [18] | Pillai D, Callen S. Pilot quality assurance programme for plasma metanephrines[J]. Ann Clin Biochem, 2010,47(Pt 2):137-142. |
| [1] | 马豆豆, 马晓彩, 常天静, 王丽芳, 丁艳, 石连杰. 临床表现似系统性红斑狼疮的大B细胞淋巴瘤骨髓受累1例[J]. 北京大学学报(医学版), 2026, 58(3): 666-669. |
| [2] | 赵业, 刁小莉, 熊焰. 细胞转移技术在微量细胞液病理诊断中的应用[J]. 北京大学学报(医学版), 2026, 58(1): 208-213. |
| [3] | 王月, 梁宇红. 繁茂型牙骨质-骨结构不良1例[J]. 北京大学学报(医学版), 2026, 58(1): 220-224. |
| [4] | 池彦廷, 蒋鸿杰, 陈艳, 徐志秀, 李斌斌. 直接免疫荧光在口腔黏膜寻常型天疱疮诊断中的价值: 基于多指标联合分析的回顾性研究[J]. 北京大学学报(医学版), 2026, 58(1): 68-73. |
| [5] | 顾静妍, 李欣艺, 赵金霞, 穆荣. 误诊为类风湿关节炎、痛风的糖尿病致Charcot关节病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1193-1197. |
| [6] | 肖晓笛, 夏有辰, 柳剑英, 付鹏. 左侧胸锁乳突肌间血管内乳头状内皮增生1例[J]. 北京大学学报(医学版), 2025, 57(5): 1002-1004. |
| [7] | 孙翔宇, 袁超, 周芯竹, 刁婧, 郑树国. 唾液微生态在口腔及全身疾病早期防治中的应用[J]. 北京大学学报(医学版), 2025, 57(5): 859-863. |
| [8] | 陈钊, 邱永康, 康磊. 经典型Sweet综合征 18F-FDG PET/CT多脏器异常显像1例[J]. 北京大学学报(医学版), 2025, 57(2): 403-407. |
| [9] | 方媛媛, 徐帆, 雷杰, 张昊, 张文宇, 孙宇, 吴宏新, 傅开元, 毛伟玉. 基于颞下颌关节紊乱病诊断标准的临床自动诊断系统的建立及验证[J]. 北京大学学报(医学版), 2025, 57(1): 192-201. |
| [10] | 车佳璐, 刘子臣, 李琨, 张晨, 车南颖. 全自动EasyNAT核酸快速检测系统检测石蜡包埋组织诊断结核病的临床价值[J]. 北京大学学报(医学版), 2024, 56(6): 1047-1051. |
| [11] | 陈心心, 唐哲, 乔艳春, 荣文笙. 北京市密云区4岁儿童患龋状况及其与龋活跃性检测的相关性[J]. 北京大学学报(医学版), 2024, 56(5): 833-838. |
| [12] | 钟华, 李原, 徐丽玲, 白明欣, 苏茵. 18F-FDG PET/CT在风湿免疫病中的应用[J]. 北京大学学报(医学版), 2024, 56(5): 853-859. |
| [13] | 李正芳,罗采南,武丽君,吴雪,孟新艳,陈晓梅,石亚妹,钟岩. 抗氨基甲酰化蛋白抗体在诊断类风湿关节炎中的应用价值[J]. 北京大学学报(医学版), 2024, 56(4): 729-734. |
| [14] | 姚海红,杨帆,唐素玫,张霞,何菁,贾园. 系统性红斑狼疮及成人Still病合并巨噬细胞活化综合征的临床特点及诊断指标[J]. 北京大学学报(医学版), 2023, 55(6): 966-974. |
| [15] | 熊焰,李鑫,梁丽,李东,鄢丽敏,李雪迎,邸吉廷,李挺. 甲状腺粗针穿刺活检病理诊断的准确性评估[J]. 北京大学学报(医学版), 2023, 55(2): 234-242. |
|
||
