北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (4): 637-641. doi: 10.19723/j.issn.1671-167X.2020.04.007
Allium覆膜金属输尿管支架长期留置治疗输尿管-回肠吻合口狭窄的初期临床经验及随访结果
董文敏1,2,王明瑞1,胡浩1,△( ),王起1,许克新1,徐涛1
),王起1,许克新1,徐涛1
- 1.北京大学人民医院泌尿外科,北京 100044
2.北京大兴区人民医院泌尿外科,北京 102600
Initial clinical experience and follow-up outcomes of treatment for ureteroileal anastomotic stricture with Allium coated metal ureteral stent
Wen-min DONG1,2,Ming-rui WANG1,Hao HU1,△(),Qi WANG1,Ke-xin XU1,Tao XU1
- 1. Department of Urology, Peking University People’s Hospital, Beijing 100044, China
2. Department of Urology, People’s Hospital of Daxing District, Beijing 102600, China
摘要:
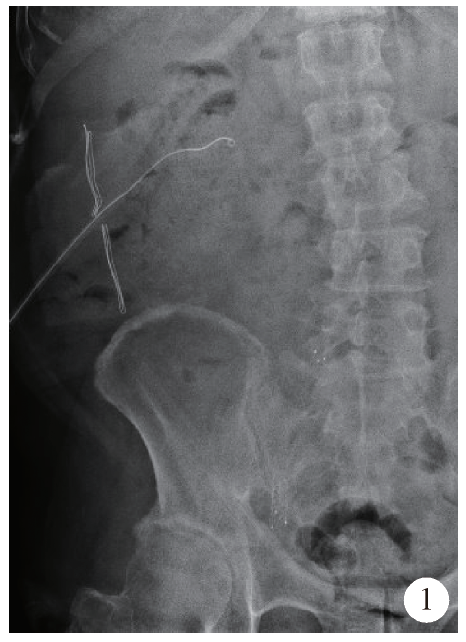
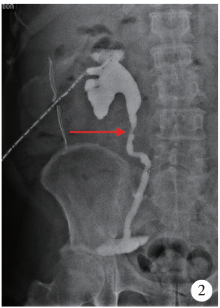
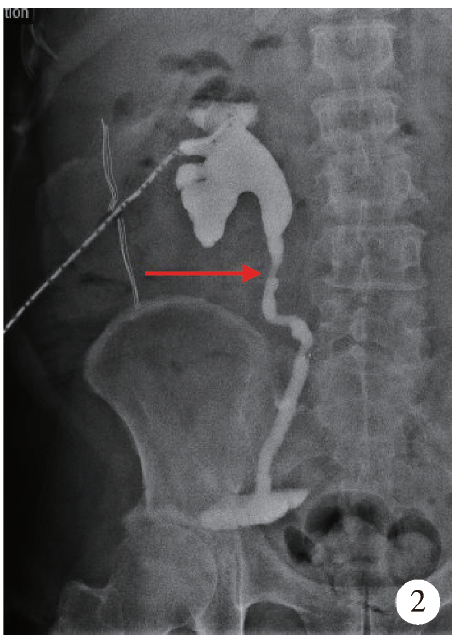
目的: 总结长期留置Allium覆膜金属输尿管支架治疗根治性膀胱切除术后输尿管-回肠吻合口狭窄的初期临床经验及随访结果。方法: 2018年9月至2019年9月在北京大学人民医院及北京市大兴区人民医院收治的8例(10侧)根治性膀胱切除术后输尿管-回肠吻合口狭窄患者,均采用Allium覆膜金属输尿管支架长期留置的方式进行输尿管狭窄的治疗。收集患者术前肾脏B超下肾盂宽度评估肾积水、手术前后肌酐及尿素氮、围手术期是否出现全身感染等手术相关和支架管相关并发症。出院后第1、3、6、12个月和之后每年复查血肌酐、尿素氮、超声下肾盂宽度,并通过尿路造影及泌尿系腹部X线检查观察支架位置和形态有无变化。回顾患者的围手术期资料和随访资料,观察统计患者的支架长期通畅率、并发症发生率、肾功能变化和肾积水情况。使用t检验或者秩和检验比较术前-末次随访的配对样本计量资料。结果: 8例患者中有6例(7侧)输尿管-回肠流出道吻合口狭窄,2例(3侧)输尿管-回肠原位新膀胱吻合口狭窄。5例患者术前长期留置输尿管单J管,平均留置时间为(20.6±8.8)个月,平均更换频率为(3.6±1.3)个月/次。术前肾脏超声检查平均肾盂宽度为(26.5±9.1) mm。6例患者采用逆行置入方式成功留置Allium输尿管支架,2例患者采用双镜联合、顺逆行结合的方式成功置入支架;围手术期未出现手术相关并发症。患者平均随访9.8个月,所有患者在末次随访时均保持Allium支架和输尿管通畅,未进行过更换或移除;与术前相比,末次随访的平均肾盂宽度和平均尿素氮均显著降低[(26.5±9.1) mm vs. (13.4±2.5) mm,P=0.008;(11.6±2.3) mmol/L vs. (10.2±2.2) mmol/L,P=0.017)],而平均血肌酐和血红蛋白均无明显差异(P>0.05);未见输尿管再梗阻、支架管移位等支架管相关并发症。结论: Allium覆膜金属输尿管支架长期留置可用于治疗输尿管-回肠吻合口狭窄,可以保持相对长期的通畅率,有助于保护肾功能,提高患者生活质量。
中图分类号:
- R693.2

| [1] |
Anderson CB, Morgan TM, Kappa S, et al. Ureteroenteric anastomotic strictures after radical cystectomy-does operative approach matter?[J]. J Urol, 2013,189(2):541-547.
doi: 10.1016/j.juro.2012.09.034 pmid: 23260561 |
| [2] | Richards KA, Cohn JA, Large MC, et al. The effect of length of ureteral resection on benign ureterointestinal stricture rate in ileal conduit or ileal neobladder urinary diversion following radical cystectomy[J]. Urol Oncol, 2015,33(2):61-65. |
| [3] |
Lobo N, Dupre S, Sahai A, et al. Getting out of a tight spot: an overview of ureteroenteric anastomotic strictures[J]. Nat Rev Urol, 2016,13(8):447-455.
doi: 10.1038/nrurol.2016.104 pmid: 27349367 |
| [4] | 林磊. 球囊扩张加双重双J管置入对良性输尿管狭窄的治疗效果观察[J]. 中国卫生标准管理, 2015,6(29):44-45. |
| [5] | 杨存让, 尹向东. 腔内三重双J管引流在输尿管狭窄治疗中的价值探讨[J]. 临床医药实践, 2008(S3):735-736. |
| [6] | 尹向军, 曹炳航, 崔文芳, 等. 双J管支架内置入应用于输尿管狭窄治疗效果分析[J]. 临床合理用药杂志, 2014,7(10):109-110. |
| [7] |
Lange D, Bidnur S, Hoag N, et al. Ureteral stent-associated complications: Where we are and where we are going[J]. Nat Rev Urol, 2015,12(1):17-25.
pmid: 25534997 |
| [8] | Bahouth Z, Moskovitz B, Halachmi S, et al. Allium stents: A novel solution for the management of upper and lower urinary tract strictures[J]. Rambam Maimonides Med J, 2017,8(4):e0043. |
| [9] | 那彦群, 叶章群, 孙颖浩. 中国泌尿外科疾病诊断治疗指南[M]. 北京: 人民卫生出版社, 2014. |
| [10] | 易宏刚. 良性输尿管狭窄的诊治现状分析[D]. 重庆: 重庆医科大学, 2018. |
| [11] |
Baten E, Akand M, Floyd MJ, et al. Evaluation of conservative approach in the management of ureteroenteric strictures following radical cystectomy with Bricker ileal conduit: a single-center experience[J]. Scand J Urol, 2016,50(6):439-444.
pmid: 27686879 |
| [12] | 李涛, 肖亚军, 邢毅飞, 等. 膀胱全切原位回肠新膀胱术后输尿管肠吻合口良性狭窄的处理[J]. 临床泌尿外科杂志, 2013,28(11):850-852. |
| [13] |
Hu W, Su B, Xiao B, et al. Simultaneous antegrade and retrograde endoscopic treatment of non-malignant ureterointestinal anastomotic strictures following urinary diversion[J]. BMC Urol, 2017,17(1):61.
pmid: 28789635 |
| [14] | Shapiro MJ, Banner MP, Amendola MA, et al. Balloon catheter dilation of ureteroenteric strictures: long-term results[J]. Radio-logy, 1988,168(2):385-387. |
| [15] |
DiMarco DS, LeRoy AJ, Thieling S, et al. Long-term results of treatment for ureteroenteric strictures[J]. Urology, 2001,58(6):909-913.
doi: 10.1016/s0090-4295(01)01420-0 pmid: 11744456 |
| [16] |
Singal RK, Denstedt JD, Razvi HA, et al. Holmium YAG laser endoureterotomy for treatment of ureteral stricture[J]. Urology, 1997,50(6):875-880.
pmid: 9426717 |
| [17] |
Leonardo C, Salvitti M, Franco G, et al. Allium stent for treatment of ureteral stenosis[J]. Minerva Urol Nefrol, 2013,65(4):277-283.
pmid: 24091480 |
| [18] |
Bahouth Z, Meyer G, Halachmi S, et al. Multicenter experience with Allium ureteral stent for the treatment of ureteral stricture and fistula[J]. Harefuah, 2015,154(12):753-756.
pmid: 26897774 |
| [19] | Guandalino M, Droupy S, Ruffion A, et al. Stent Allium urétéral dans la prise en charge des sténoses urétérales. Étude rétrospective multicentrique[J]. Progrès en Urologie, 2017,27(1):26-32. |
| [20] | Moskovitz B, Halachmi S, Nativ O. A new self-expanding, large-caliber ureteral stent: Results of a multicenter experience[J]. J Endourol, 2012,26(11):1523-1527. |
| [1] | 杜文, 章文博, 于尧, 刘硕, 苏惠裕, 胡耒豪, 唐祖南, 吴彬彰, 陈震, 李家琦, 王昊, 彭歆. 口腔颌面部肿瘤"数智化外科"诊疗流程探索与临床应用[J]. 北京大学学报(医学版), 2026, 58(2): 278-284. |
| [2] | 武竞衡, 薛云皓, 陈山林, 郭银涛, 刘云涛, 张维. 超显微淋巴管-静脉吻合术治疗肢体淋巴水肿: 基于临床分期与吲哚菁绿分型的疗效分析[J]. 北京大学学报(医学版), 2026, 58(2): 359-364. |
| [3] | 刘嘉昱, 祝宁, 张育祯, 高贤明, 张宇. 动态导航辅助环钻取骨的准确性[J]. 北京大学学报(医学版), 2026, 58(2): 365-371. |
| [4] | 李斌, 梁寒. 机器人胃癌根治术:研究进展与实践挑战[J]. 北京大学学报(医学版), 2026, 58(2): 416-422. |
| [5] | FarinEbrahimi, 冯志强, FarazEbrahimi, 韩玮华, 于子杨, 贾宽宽, 安金刚. 上颌药物相关性颌骨坏死的不同分期手术治疗效果[J]. 北京大学学报(医学版), 2026, 58(1): 107-114. |
| [6] | 于录, 吴灵, 刘筱菁, 李自力. 基于数据库相似性检索的正颌外科手术规划技术流程可行性研究: 随机对照试验[J]. 北京大学学报(医学版), 2026, 58(1): 145-152. |
| [7] | 王晓林, 郭邵逸, 陈大召, 温锡杰, 华勇, 张亮, 张秦. 全髋关节置换术治疗系统性红斑狼疮继发股骨头缺血性坏死的随访研究[J]. 北京大学学报(医学版), 2025, 57(6): 1081-1088. |
| [8] | 李慎谟, 苏丹丹, 林己煜, 宋昊东, 马潞林, 侯小飞, 王国良, 张洪宪, 叶剑飞, 张树栋. 腹腔镜下膀胱癌根治术同期行肾输尿管全长切除术的预后分析[J]. 北京大学学报(医学版), 2025, 57(5): 961-966. |
| [9] | 左超, 王国立, 杨昆霖, 车新艳, 孟一森, 张凯. 前列腺体积不同的患者经尿道光纤铥激光前列腺剜除术的有效性及安全性比较[J]. 北京大学学报(医学版), 2025, 57(4): 711-716. |
| [10] | 黄万伟, 沙显燊, 张艺宝, 伍国豪, 骆峰, 陈智慧, 叶东明, 李学松, 赖彩永. 完全3D腹腔镜回肠代双侧输尿管联合膀胱扩大术修复放射治疗后双侧输尿管狭窄并膀胱挛缩[J]. 北京大学学报(医学版), 2025, 57(4): 789-795. |
| [11] | 赵兆, 张维宇, 杨文博, 张勇杰, 张晓鹏, 赵慧颖, 周刚, 王强. 低龄、低体重儿童肾移植2例[J]. 北京大学学报(医学版), 2025, 57(4): 803-807. |
| [12] | 杨源源, 张珊珊, 俞光岩, 杨辉俊, 杨宏宇. 部分下颌下腺切除术治疗下颌下腺良性肿瘤的临床效果[J]. 北京大学学报(医学版), 2025, 57(2): 334-339. |
| [13] | 刘振龙, 侯振宸, 胡晓青, 任爽, 郭秦炜, 徐雁, 龚熹, 敖英芳. 关节镜下组织工程支架修复软骨损伤[J]. 北京大学学报(医学版), 2025, 57(2): 384-387. |
| [14] | 胡轶博, 吕伟佳, 夏炜, 刘亦洪. 基于细胞生长与成骨分化的不同孔径生物支架流体力学有限元分析[J]. 北京大学学报(医学版), 2025, 57(1): 97-105. |
| [15] | 王明瑞, 王起, 胡浩, 赖金惠, 唐鑫伟, 万春艳, 许克新, 徐涛. 覆膜金属输尿管支架治疗盆腔脂肪增多症所致肾积水的疗效[J]. 北京大学学报(医学版), 2024, 56(5): 919-922. |
|
||
