北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (4): 667-671. doi: 10.19723/j.issn.1671-167X.2020.04.013
经皮肾镜去石术后出血的介入治疗
高健1,△( ),胡立宝1,陈尘1,郅新1,徐涛2,△()
),胡立宝1,陈尘1,郅新1,徐涛2,△()
- 1.北京大学人民医院 放射科,北京 100044
2.北京大学人民医院 泌尿外科,北京 100044
Interventional treatment of hemorrhage after percutaneous nephrolithotomy
Jian GAO1,△(),Li-bao HU1,Chen CHEN1,Xin ZHI1,Tao XU2,△()
- 1. Department of Radiology, Peking University People’s Hospital, Beijing 100044, China
2. Department of Urology, Peking University People’s Hospital, Beijing 100044, China
摘要:
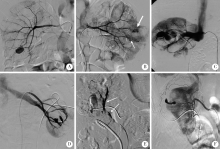
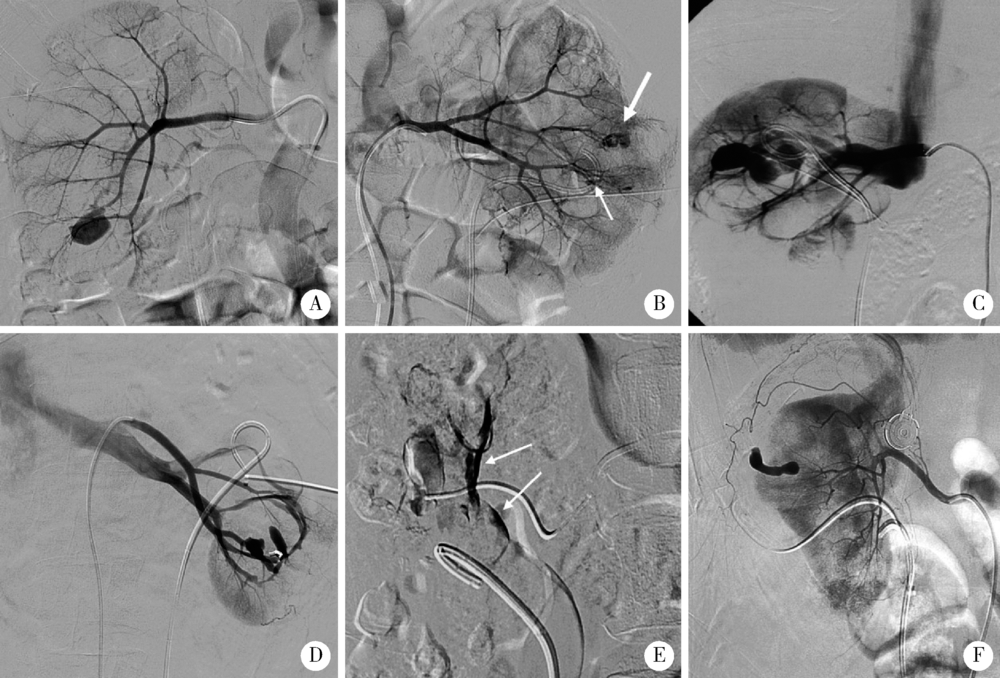
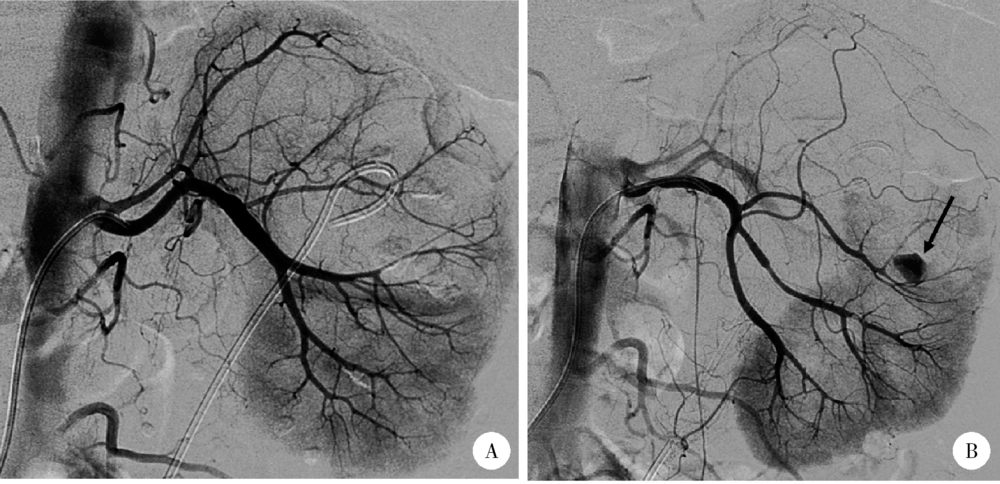
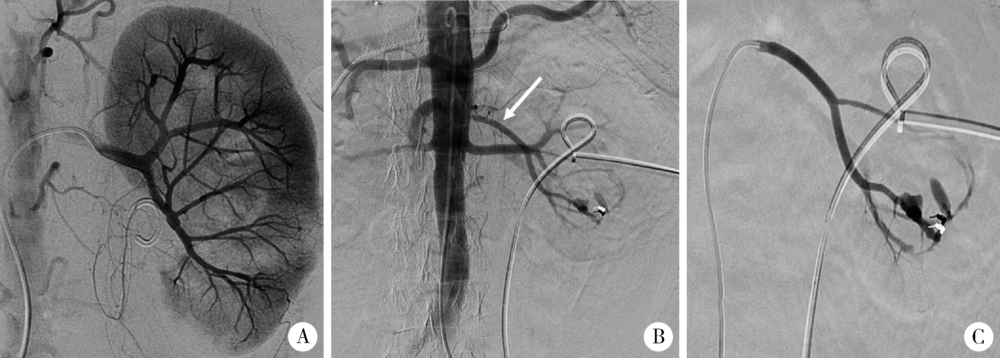
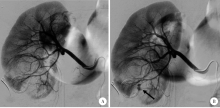
目的: 研究超选择性肾动脉栓塞在治疗经皮肾镜术后出血中的效果及失败原因。方法: 对65例伴有血液动力学改变的经皮肾镜术后出血患者行肾动脉造影,用微导管行超选择性插管,用微弹簧圈栓塞损伤动脉。若首次肾动脉造影无阳性发现,则采用以下措施以防止遗漏病灶:(1)腹主动脉造影;(2)重复肾动脉造影;(3)造瘘管走行区域肾动脉分支超选择造影;(4)保留穿刺通道,拔除肾造瘘管后造影。对肾动脉出血的造影表现进行总结,并对栓塞止血失败的原因进行分析。结果: 65例患者中,造影有阳性发现的60例(62个肾脏), 均经超选择性栓塞成功止血。肾动脉造影的阳性表现包括:假性动脉瘤形成、斑片状造影剂外溢、假性动脉瘤合并动静脉瘘、造影剂进入集合系统、造影剂弥散至肾被膜下。一次栓塞成功53例(55个肾脏), 成功率88.71%,两次栓塞成功率96.77%。首次栓塞失败的原因主要是遗漏病灶(4例,57.10%)和栓塞的受损血管再通(2例,28.57%)。5例患者肾动脉造影无阳性发现,经保守治疗血尿停止。所有患者介入治疗后3、6、12个月随访,均未再次出现血尿,且未发生持续、严重的肾功能损害。结论: 超选择肾动脉栓塞是治疗经皮肾镜术后出血的有效方法,肾动脉造影遗漏病灶是造成止血失败的主要原因。
中图分类号:
- R814.47





| [1] | Un S, Cakir V, Kara C, et al. Risk factors for hemorrhage requiring embolization after percutaneous nephrolithotomy[J]. Can Urol Assoc J, 2015,9(9/10):594-598. |
| [2] | El Tayeb MM, Knoedler JJ, Krambeck AE, et al. Vascular complications after percutaneous nephrolithotomy: 10 years of expe-rience[J]. Urology, 2015,85(4):777-781. |
| [3] | El-Nahas AR, Shokeir AA, Mohsen T, et al. Functional and morphological effects of postpercutaneous nephrolithotomy superselective renal angiographic embolization[J]. Urology, 2008,71(3):408-412. |
| [4] | Kervancioglu S, Gelebek Yilmaz F, Erturhan S. Endovascular management of vascular complications after percutaneous nephrolithotomy[J]. Vasa, 2014,43(6):459-464. |
| [5] | Li L, Zhang Y, Chen Y, et al. A multicentre retrospective study of transcatheter angiographic embolization in the treatment of delayed haemorrhage after percutaneous nephrolithotomy[J]. Eur Radiol, 2015,25(4):1140-1147. |
| [6] | Wang HL, Xu CY, Wang HH, et al. Emergency transcatheter arterial embolization for acute renal hemorrhage[J]. Medicine, 2015,94(42):e1667. |
| [7] | Choi MJ, Kim PH, Shin JH, et al. Angiographic management of percutaneous renal procedure-related bleeding: A single-center experience[J]. Int J Urol, 2019,26(3):406-412. |
| [8] |
El-Nahas AR, Shokeir AA, El-Assmy AM, et al. Postpercuta-neous nephrolithotomy extensive hemorrhage: A study of risk factors[J]. J Urol, 2007,177(2):576-579.
pmid: 17222636 |
| [9] | 任医民, 伍筱梅, 温宇, 等. 经皮肾镜取石术后肾出血栓塞失败的原因分析[J]. 中华医学杂志, 2017,97(1):22-25. |
| [10] |
He ZH, Lei HQ, Lu XB, et al. Analysis of repeated renal arte-riography after percutaneous nephrolithotomy[J]. Urolithiasis, 2017,45(5):495-499.
pmid: 27837249 |
| [11] | Ding XB, Guan JJ, Tian JY, et al. Subcostal artery bleeding after percutaneous nephrolithotomy: A case report and literature review[J]. J Int Med Res, 2018,46(10):4350-4353. |
| [12] | Seetharama MK, Ananthashayana VH, Shivanand G, et al. Interventional radiology in the management of visceral artery pseudo-aneurysms: A review of techniques and embolic materials[J]. Korean J Radiol, 2016,17(3):351-363. |
| [13] | Ganpule AP, Shah DH, Desai MR. Postpercutaneous nephrolithotomy bleeding: Aetiology and management[J]. Curr Opin Urol, 2014,24(2):189-194. |
| [14] | 熊六林, 黄晓波, 叶雄俊, 等. 经皮肾镜术后肾脏严重出血特点及选择性介入栓塞的时机选择(附13例报告)[J]. 北京大学学报(医学版), 2010,42(4):465-468. |
| [1] | 孟庆伟, 范梦, 郭煌达, 章涵宇, 王梦莹, 王斯悦, 彭和香, 王雪珩, 侯天姣, 秦雪英, 陈大方, 李劲, 武轶群, 吴涛, 陈洪波, 胡永华. 老年人心源性卒中抗凝治疗的预后[J]. 北京大学学报(医学版), 2026, 58(3): 536-542. |
| [2] | 王晓林, 郭邵逸, 陈大召, 温锡杰, 华勇, 张亮, 张秦. 全髋关节置换术治疗系统性红斑狼疮继发股骨头缺血性坏死的随访研究[J]. 北京大学学报(医学版), 2025, 57(6): 1081-1088. |
| [3] | 左超, 王国立, 杨昆霖, 车新艳, 孟一森, 张凯. 前列腺体积不同的患者经尿道光纤铥激光前列腺剜除术的有效性及安全性比较[J]. 北京大学学报(医学版), 2025, 57(4): 711-716. |
| [4] | 赵兆, 张维宇, 杨文博, 张勇杰, 张晓鹏, 赵慧颖, 周刚, 王强. 低龄、低体重儿童肾移植2例[J]. 北京大学学报(医学版), 2025, 57(4): 803-807. |
| [5] | 郭华秋, 王哲, 杨雪, 白洁. 口腔急诊出血患者的临床特征与危险因素[J]. 北京大学学报(医学版), 2025, 57(1): 142-147. |
| [6] | 丁艳, 李超然, 黄文生, 朱林忠, 王丽芳, 马豆豆, 张娟, 石连杰. 有肾脏意义单克隆免疫球蛋白血症继发lgA血管炎并导致小肠坏死1例[J]. 北京大学学报(医学版), 2024, 56(6): 1101-1105. |
| [7] | 丁汉东, 王琴, 廖贵益, 郝宗耀. 肾移植术后并发消化道出血的诊治[J]. 北京大学学报(医学版), 2024, 56(5): 902-907. |
| [8] | 侯婉音,董捷. 腹膜透析患者获得性肾囊肿出血3例[J]. 北京大学学报(医学版), 2024, 56(3): 546-550. |
| [9] | 司筱芊,赵秀娟,朱凤雪,王天兵. 创伤出血性休克后急性呼吸窘迫综合征的危险因素[J]. 北京大学学报(医学版), 2024, 56(2): 307-312. |
| [10] | 陈克伟,邓绍晖,刘茁,张洪宪,马潞林,张树栋. 肾血管平滑肌脂肪瘤破裂出血的手术时机[J]. 北京大学学报(医学版), 2024, 56(2): 326-331. |
| [11] | 冯敏,陈哲,程永静. 以十二指肠溃疡为突出表现的IgG4相关性疾病1例[J]. 北京大学学报(医学版), 2023, 55(6): 1125-1129. |
| [12] | 兰东,刘茁,李宇轩,王国良,田晓军,马潞林,张树栋,张洪宪. 根治性肾切除和静脉癌栓取出术大出血的危险因素[J]. 北京大学学报(医学版), 2023, 55(5): 825-832. |
| [13] | 田聪,刘军,杨波,乔佳佳,黄晓波,许清泉. 经皮肾镜取石术中异常肾盂黏膜活检结果分析[J]. 北京大学学报(医学版), 2023, 55(5): 948-952. |
| [14] | 许素环,王蓓蓓,庞秋颖,钟丽君,丁炎明,黄燕波,车新艳. 等体温膀胱冲洗对经尿道前列腺电切术患者干预效果的meta分析[J]. 北京大学学报(医学版), 2023, 55(4): 676-683. |
| [15] | 李辉,高阳旭,王书磊,姚红新. 恶性肿瘤患儿完全植入式静脉输液港手术并发症[J]. 北京大学学报(医学版), 2022, 54(6): 1167-1171. |
|
||
