北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (1): 188-194. doi: 10.19723/j.issn.1671-167X.2021.01.028
肺叶切除术中少尿与术后急性肾损伤的关系
孟昭婷,穆东亮( )
)
- 北京大学第一医院麻醉科,北京 100034
Impact of oliguria during lung surgery on postoperative acute kidney injury
MENG Zhao-ting,MU Dong-liang()
- Department of Anesthesiology, Peking University First Hospital, Beijing 100034, China
摘要:
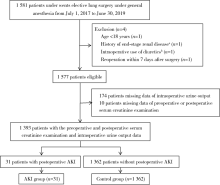
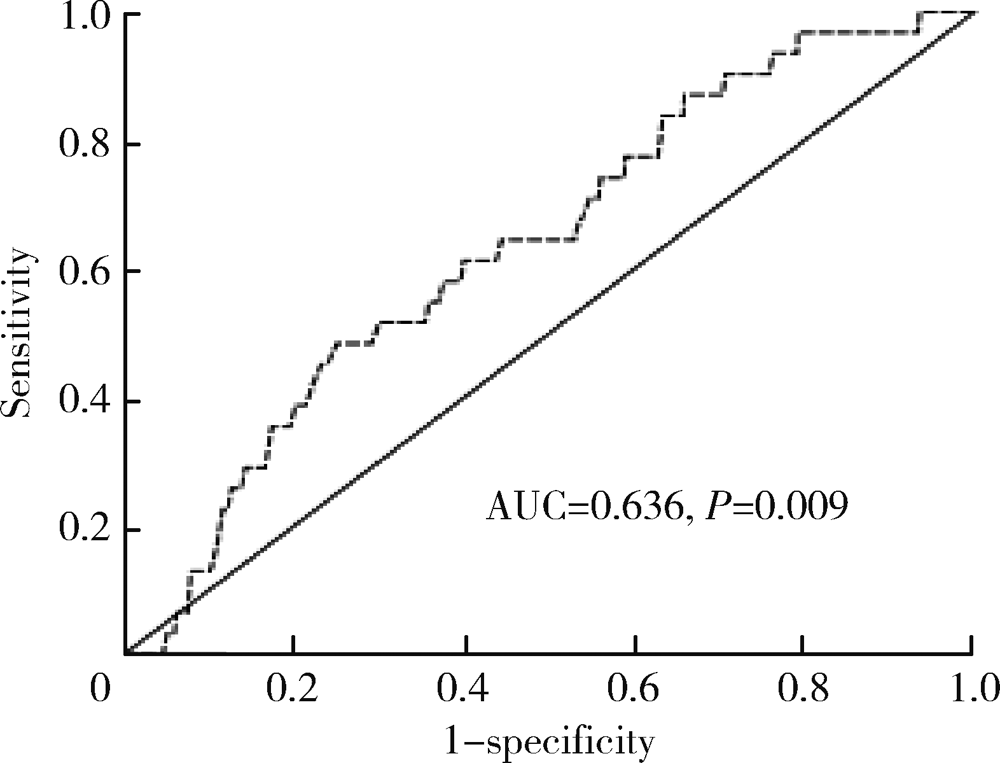
目的: 探索术中尿量对术后急性肾损伤(acute kidney injury, AKI)的影响,以及术后AKI发生的独立危险因素。方法: 选择2017年7月至2019年6月于北京大学第一医院在全身麻醉下接受择期肺叶切除术的患者作为研究对象进行回顾性队列研究。将入组患者按照是否发生术后AKI分为AKI组和对照组。首先对围术期各变量进行单因素分析,探讨其与术后AKI的关系;其次,采用受试者工作特征曲线(receiver operating characteristic curve,ROC curve)分析术中尿量对术后AKI的预测价值,并以约登(Youden)指数为最大值时的上下4个界值[以0.1 mL/(kg·h)为间隔]为少尿界值,采用单因素分析探索各界值定义下的少尿与AKI发生风险的关系,并取OR值最大者为少尿界值;最后,将单因素分析中P<0.10的围术期各变量共同代入多因素Logistic回归模型,分析术后AKI的独立危险因素。结果: 共1 393名患者最终纳入研究,术后AKI发生率为2.2%。ROC曲线显示术中单位尿量用于预测术后AKI的曲线下面积为0.636(P=0.009), 约登指数为最大值时(约登指数0.234,敏感度48.4%,特异度75.0%)的少尿界值为0.785 mL/(kg·h)。进一步取0.7、0.8、0.9、1.0 mL/(kg·h)以及传统界值0.5 mL/(kg·h)为少尿界值分析少尿对术后AKI的影响。单因素分析显示,以小于0.8 mL/(kg·h)为少尿界值时,少尿患者发生AKI的风险增加最为显著(OR=2.774, 95%CI 1.357~5.671, P=0.004)。多因素回归分析显示术中尿量<0.8 mL/(kg·h)(OR=2.698,95%CI 1.260~5.778, P=0.011)是术后AKI发生的独立危险因素,另两个独立危险因素为术前血红蛋白≤120.0 g/L(OR=3.605, 95%CI 1.545~8.412, P=0.003)以及术前估计肾小球滤过率<30 mL/(min·1.73 m2)(OR=11.009, 95%CI 1.813~66.843, P=0.009)。 结论: 对于肺叶切除术,术中少尿是术后AKI发生的独立危险因素,且尿量<0.8 mL/(kg·h)是可能的筛选标准。
中图分类号:
- R614


| [1] | Nadim MK, Forni LG, Bihorac A, et al. Cardiac and vascular surgery-associated acute kidney injury: the 20th International Consensus Conference of the ADQI (acute disease quality initiative) group[J]. J Am Heart Assoc, 2018,7(11):e8834. |
| [2] |
Sanaiha Y, Kavianpour B, Dobaria V, et al. Acute kidney injury is independently associated with mortality and resource use after emergency general surgery operations[J]. Surgery, 2020,167(2):328-334.
doi: 10.1016/j.surg.2019.07.035 pmid: 31668777 |
| [3] |
Vaara ST, Bellomo R. Postoperative renal dysfunction after noncardiac surgery[J]. Curr Opin Crit Care, 2017,23(5):440-446.
doi: 10.1097/MCC.0000000000000439 pmid: 28820797 |
| [4] |
Grams ME, Sang Y, Coresh J, et al. Acute kidney injury after major surgery: a retrospective analysis of veterans health administration data[J]. Am J Kidney Dis, 2016,67(6):872-880.
doi: 10.1053/j.ajkd.2015.07.022 pmid: 26337133 |
| [5] | Cardinale D, Cosentino N, Moltrasio M, et al. Acute kidney injury after lung cancer surgery: Incidence and clinical relevance, predictors, and role of N-terminal pro B-type natriuretic peptide[J]. Lung Cancer, 2018,123(9):155-159. |
| [6] |
Ostermann M, Joannidis M. Acute kidney injury 2016: diagnosis and diagnostic workup[J]. Crit Care, 2016,20(1):299-311.
doi: 10.1186/s13054-016-1478-z pmid: 27670788 |
| [7] |
Weiss R, Meersch M, Pavenstädt HJ, et al. Acute kidney injury: a frequently underestimated problem in perioperative medicine[J]. Dtsch Arztebl Int, 2019,116(49):833-842.
doi: 10.3238/arztebl.2019.0833 pmid: 31888797 |
| [8] |
Zarbock A, Koyner JL, Hoste EAJ, et al. Update on perioperative acute kidney injury[J]. Anesth Analg, 2018,127(5):1236-1245.
doi: 10.1213/ANE.0000000000003741 pmid: 30138176 |
| [9] |
du Toit L, Biccard BM. The relationship between intraoperative oliguria and acute kidney injury[J]. Br J Anaesth, 2019,122(6):707-710.
doi: 10.1016/j.bja.2019.03.008 pmid: 30961912 |
| [10] |
Hori D, Katz1 NM, Fine DM, et al. Defining oliguria during cardiopulmonary bypass and its relationship with cardiac surgery-associated acute kidney injury[J]. Br J Anaesth, 2016,117(6):733-740.
pmid: 27956671 |
| [11] |
Mizota T, Yamamoto Y, Hamada M, et al. Intraoperative oliguria predicts acute kidney injury after major abdominal surgery[J]. Br J Anaesth, 2017,119(6):1127-1134.
doi: 10.1093/bja/aex255 pmid: 29136086 |
| [12] |
Kim HJ, Cha SI, Kim CH, et al. Risk factors of postoperative acute lung injury following lobectomy for nonsmall cell lung cancer[J]. Medicine, 2019,98(13):e15078.
doi: 10.1097/MD.0000000000015078 pmid: 30921242 |
| [13] |
O’Connor ME, Kirwan CJ, Pearse RM, et al. Incidence and associations of acute kidney injury after major abdominal surgery[J]. Intensive Care Med, 2016,42(4):521-530.
doi: 10.1007/s00134-015-4157-7 pmid: 26602784 |
| [14] |
Levey AS, Coresh J, Greene T, et al. Expressing the modification of diet in renal disease study equation for estimating glomerular filtration rate with standardized serum creatinine values[J]. Clin Chem, 2007,53(4):766-772.
doi: 10.1373/clinchem.2006.077180 pmid: 17332152 |
| [15] |
Quan S, Pannu N, Wilson T, et al. Prognostic implications of adding urine output to serum creatinine measurements for staging of acute kidney injury after majorsurgery: a cohort study[J]. Nephrol Dial Transplant, 2016,31(12):2049-2056.
doi: 10.1093/ndt/gfw374 pmid: 27941063 |
| [16] |
Kellum JA, Sileanu FE, Murugan R, et al. Classifying AKI by urine output versus serum creatinine level[J]. J Am Soc Nephrol, 2015,26(9):2231-2238.
doi: 10.1681/ASN.2014070724 pmid: 25568178 |
| [17] |
Eknoyan G. Rufus of ephesus and his “diseases of the kidneys”[J]. Nephron, 2002,91(3):383-390.
doi: 10.1159/000064277 pmid: 12119467 |
| [18] |
Macedo E, Malhotra R, Bouchard J, et al. Oliguria is an early predictor of higher mortality in critically ill patients[J]. Kidney Int, 2011,80(7):760-770.
doi: 10.1038/ki.2011.150 pmid: 21716258 |
| [19] | Inácio R, Gameiro J, Amaro S, et al. Intraoperative oliguria does not predict postoperative acute kidney injury in major abdominal surgery: a cohort analysis [J/OL]. J Bras Nefrol[2019-12-01]. https://doi.org/10.1590/2175-8239-jbn-2019-0244. |
| [20] |
Rung GW, Marshall WK. Nerve blocks in the critical care environment[J]. Crit Care Clin, 1990,6(2):343-367.
pmid: 2188709 |
| [21] |
Matot I, Dery E, Bulgov Y, et al. Fluid management during video-assisted thoracoscopic surgery for lung resection: a ran-domized, controlled trial of effects on urinary output and postoperative renal function[J]. J Thorac Cardiovasc Surg, 2013,146(2):461-466.
doi: 10.1016/j.jtcvs.2013.02.015 pmid: 23558303 |
| [22] |
Myles PS, Bellomo R, Corcoran T, et al. Restrictive versus liberal fluid therapy for major abdominal surgery[J]. N Engl J Med, 2018,378(24):2263-2274.
doi: 10.1056/NEJMoa1801601 pmid: 29742967 |
| [1] | 魏慧, 张警丰, 姚中强, 赵金霞. 类风湿关节炎合并慢性病贫血患者的临床特征及相关因素[J]. 北京大学学报(医学版), 2026, 58(2): 307-312. |
| [2] | 赵杰, 付春, 赵秀娟, 薛海岩, 李纾, 王振洲, 朱凤雪. 胸部创伤患者在重症监护病房内发生呼吸机相关性肺炎的危险因素[J]. 北京大学学报(医学版), 2026, 58(2): 351-358. |
| [3] | 郭芷均, 俎明, 马超, 张贺军, 张静, 丁士刚. 同时性多发早期胃癌漏诊病灶的临床病理特征[J]. 北京大学学报(医学版), 2026, 58(2): 410-415. |
| [4] | 李博闻, 张强, 孙益鑫. 儿童及青年漏斗胸患者Nuss术后发生脊柱侧弯的风险预测模型建立及验证[J]. 北京大学学报(医学版), 2025, 57(5): 941-946. |
| [5] | 杨小勇, 张帆, 马潞林, 刘承. 前列腺导管腺癌临床特征及腺外侵犯的影响因素[J]. 北京大学学报(医学版), 2025, 57(5): 956-960. |
| [6] | 刘伟, 郭稳, 过哲, 李春艳, 李云龙, 刘思奇, 张亮, 宋慧. 痛风患者放射学阴性骨侵蚀的相关危险因素[J]. 北京大学学报(医学版), 2025, 57(4): 735-739. |
| [7] | 陆梦溪, 刘秋萍, 周恬静, 刘晓非, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 基于社区人群队列的甘油三酯-葡萄糖指数与心血管病发病和死亡的关联[J]. 北京大学学报(医学版), 2025, 57(3): 430-435. |
| [8] | 杨龙傲, 金旭, 黄文初, 何丽华, 陈娟. 视屏作业人员视疲劳及干眼的流行病学调查[J]. 北京大学学报(医学版), 2025, 57(3): 554-561. |
| [9] | 郭华秋, 王哲, 杨雪, 白洁. 口腔急诊出血患者的临床特征与危险因素[J]. 北京大学学报(医学版), 2025, 57(1): 142-147. |
| [10] | 邓敏婷, 王楠, 夏斌, 赵玉鸣, 朱俊霞. 儿童及青少年挫入恒前牙自行再萌出的相关影响因素[J]. 北京大学学报(医学版), 2025, 57(1): 148-153. |
| [11] | 李钰锴, 王红彦, 罗靓, 李云, 李春. 抗磷脂抗体在白塞病合并血栓中的临床意义[J]. 北京大学学报(医学版), 2024, 56(6): 1036-1040. |
| [12] | 田杨, 韩永正, 李娇, 王明亚, 曲音音, 房景超, 金辉, 李民, 王军, 徐懋, 王圣林, 郭向阳. 颈椎前路手术后硬膜外血肿的发生率和危险因素[J]. 北京大学学报(医学版), 2024, 56(6): 1058-1064. |
| [13] | 王明瑞, 赖金惠, 姬家祥, 唐鑫伟, 胡浩浦, 王起, 许克新, 徐涛, 胡浩. 使用中文版威斯康星结石生活质量问卷预测肾结石患者生活质量降低的危险因素[J]. 北京大学学报(医学版), 2024, 56(6): 1069-1074. |
| [14] | 李志存, 吴天俣, 梁磊, 范宇, 孟一森, 张骞. 穿刺活检单针阳性前列腺癌术后病理升级的危险因素分析及列线图模型构建[J]. 北京大学学报(医学版), 2024, 56(5): 896-901. |
| [15] | 颜野,李小龙,夏海缀,朱学华,张羽婷,张帆,刘可,刘承,马潞林. 前列腺癌根治术后远期膀胱过度活动症的危险因素[J]. 北京大学学报(医学版), 2024, 56(4): 589-593. |
|
||
