北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (5): 946-951. doi: 10.19723/j.issn.1671-167X.2021.05.023
全身麻醉下小儿开颅术术中心脏前负荷动态指标的一致性分析
刘雅菲1,宋琳琳1,△( ),邢茂炜1,蔡立新2,王东信1
),邢茂炜1,蔡立新2,王东信1
- 北京大学第一医院1. 麻醉科, 北京 100034
2.儿童癫痫中心, 北京 100034
Comparison of pulse pressure variation, stroke volume variation, and plethysmographic variability index in pediatric patients undergoing craniotomy
LIU Ya-fei1,SONG Lin-lin1,△(),XING Mao-wei1,CAI Li-xin2,WANG Dong-xin1
- 1. Department of Anesthesiology, Beijing 100034, China
2. Pediatric Epilepsy Center, Peking University First Hospital, Beijing 100034, China
摘要:
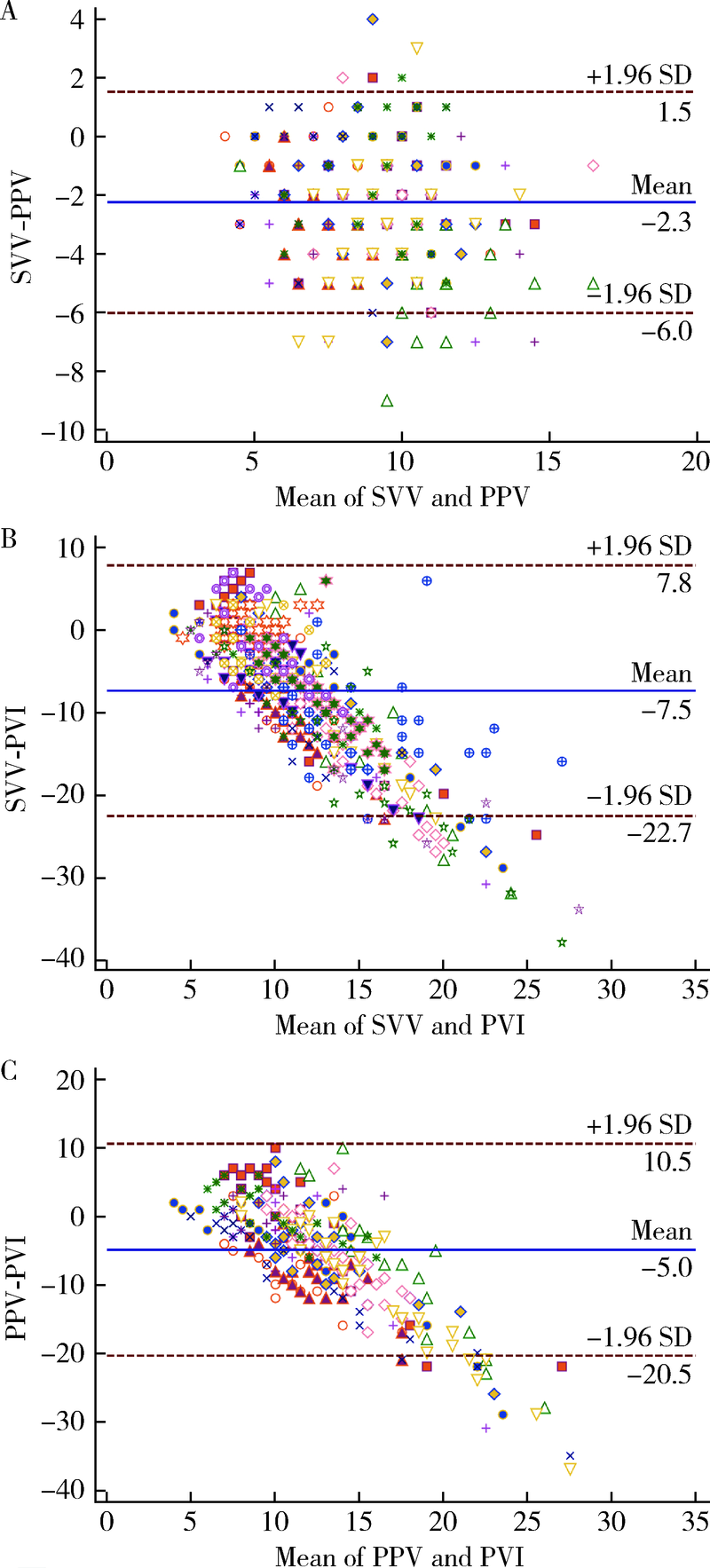
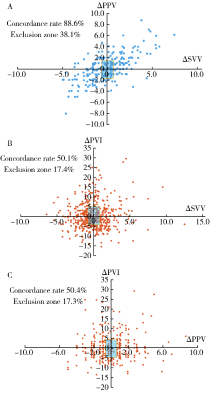
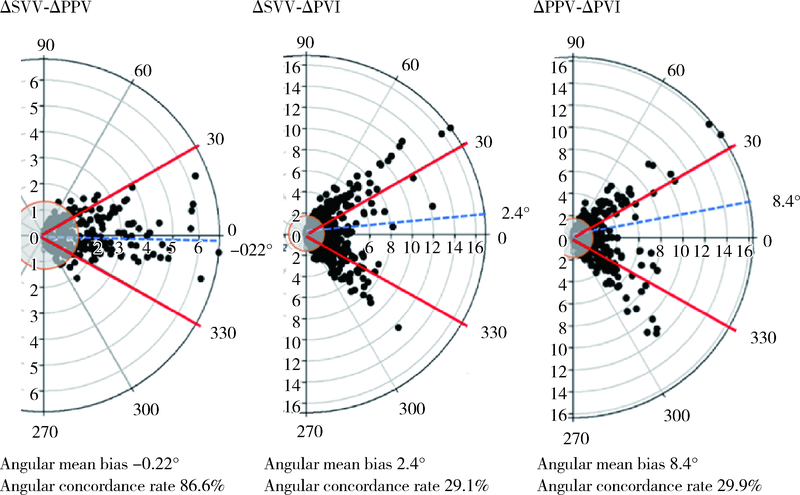
目的: 在小儿开颅癫痫病灶切除术中连续监测每搏量变异(stroke volume variation, SVV)、脉压变异(pulse pressure variation, PPV)和脉搏容积变异(plethysmographic variability index, PVI)3项心脏前负荷动态指标,评价这些常用动态指标的一致性,探索三者之间是否可以互换,以简化临床决策过程。方法: 30例行择期开颅癫痫病灶切除术的0 ~ 14岁患儿术中常规监测SVV、PPV和PVI, 根据上述指标和动脉收缩压实施目标导向液体管理。所有数据对分为6个阶段,每个阶段选取3 ~ 8个数据对,用Bland-Altman法分析数据对数值的一致性,用四象限图和极图分析数据对的同向变化趋势。结果: 患儿术中动脉收缩压为 (94±19) mmHg,平均SVV、PPV和PVI分别为8%±2%、10%±3%和15%±7%,共分析834个数据对。Bland-Altman分析显示SVV-PPV的平均偏倚为-2.3,一致限为-6.0 ~ 1.5,误差百分比为26%。SVV-PVI和PPV-PVI的平均偏倚分别为-7.5和-5.0,一致限分别为-22.7 ~ 7.8和-20.5 ~ 10.5,误差百分比分别为54%和43%。四象限图分析中3项指标变化的符合率分别为ΔSVV-ΔPPV 88.6%、ΔSVV-ΔPVI 50.1%、ΔPPV-ΔPVI 50.4%。<3岁者PPV-SVV符合率高于≥ 3岁者(92.7%与84.2%)。极坐标图分析中SVV-PPV变化的角符合率为86.6%,基于动脉压力波形的指标(SVV和PPV)与PVI变化符合率较差(分别为29.1%和29.9%)。结论: 小儿开颅术中SVV和PPV变化趋势一致性较高,尤其<3岁者,二者可以互换,无需额外使用SVV监测设备;但基于动脉压力波形的指标(SVV和PPV)与PVI之间变化趋势的一致性较差,不能互换。联合PPV和PVI用于监测心脏前负荷可能有助于提高小儿术中补液反应性的预测值。
中图分类号:
- R726.1



| [1] |
Chen PH, Chan KC, Liao MH, et al. Accuracy of dynamic preload variables for predicting fluid responsiveness in patients with pediatric liver cirrhosis: a prospective study [J]. Paediatr Anaesth, 2020, 30(4):455-461.
doi: 10.1111/pan.v30.4 |
| [2] |
Cheng YW, Xu F, Li J. Identification of volume parameters monitored with a noninvasive ultrasonic cardiac output monitor for predicting fluid responsiveness in children after congenital heart disease surgery [J]. Medicine (Baltimore), 2018, 97(39):e12289.
doi: 10.1097/MD.0000000000012289 |
| [3] |
Liu T, Xu C, Wang M, et al. Reliability of pleth variability index in predicting preload responsiveness of mechanically ventilated patients under various conditions: a systematic review and meta-analysis [J]. BMC Anesthesiol, 2019, 19(1):67.
doi: 10.1186/s12871-019-0744-4 |
| [4] |
Kim DH, Shin S, Kim JY, et al. Pulse pressure variation and pleth variability index as predictors of fluid responsiveness in patients undergoing spinal surgery in the prone position [J]. Ther Clin Risk Manag, 2018, 14:1175-1183.
doi: 10.2147/TCRM |
| [5] |
Saugel B, Heeschen J, Hapfelmeier A, et al. Cardiac output estimation using multi-beat analysis of the radial arterial blood pressure waveform: a method comparison study in patients having off-pump coronary artery bypass surgery using intermittent pulmonary artery thermodilution as the reference method [J]. J Clin Monit Comput, 2020, 34(4):649-654.
doi: 10.1007/s10877-019-00375-z pmid: 31456072 |
| [6] | Monnet X, Marik PE, Teboul JL. Prediction of fluid responsiveness: an update [J]. Ann Intensive Care, 2016, 2016(6):111. |
| [7] |
Joosten A, Jacobs A, Desebbe O, et al. Monitoring of pulse pressure variation using a new smartphone application (Capstesia) versus stroke volume variation using an uncalibrated pulse wave analysis monitor: a clinical decision making study during major abdominal surgery [J]. J Clin Monit Comput, 2019, 33(5):787-793.
doi: 10.1007/s10877-018-00241-4 |
| [8] |
Ji SH, Song IK, Jang YE, et al. Comparison of pulse pressure variation and pleth variability index in the prone position in pediatric patients under 2 years old [J]. Korean J Anesthesiol, 2019, 72(5):466-471.
doi: 10.4097/kja.19128 |
| [9] |
Desgranges FP, Evain JN, Pereira de Souza NE, et al. Does the plethysmographic variability index predict fluid responsiveness in mechanically ventilated children? A meta-analysis [J]. Br J Anaesth, 2016, 117(3):409-410.
doi: 10.1093/bja/aew245 pmid: 27543550 |
| [10] |
Lee JH, Kim EH, Jang YE, et al. Fluid responsiveness in the pediatric population [J]. Korean J Anesthesiol, 2019, 72(5):429-440.
doi: 10.4097/kja.19305 |
| [1] | 李宗瀚, 黄洋阅, 李宁, 李明磊, 宋宏程, 张潍平, 刘超. 国产单孔蛇形臂机器人手术系统在儿童肾盂成形术中的应用[J]. 北京大学学报(医学版), 2025, 57(4): 662-665. |
| [2] | 赵兆, 张维宇, 杨文博, 张勇杰, 张晓鹏, 赵慧颖, 周刚, 王强. 低龄、低体重儿童肾移植2例[J]. 北京大学学报(医学版), 2025, 57(4): 803-807. |
| [3] | 张依航, 蔡珊, 陈子玥, 刘云飞, 党佳佳, 师嫡, 李佳欣, 黄天彧, 宋逸. 基于RE-AIM框架儿童青少年近视与肥胖共病综合干预实施性研究结局指标的构建[J]. 北京大学学报(医学版), 2025, 57(3): 436-441. |
| [4] | 唐孟利, 刘扬, 秦冉, 郭欣, 李宏田. 我国10省幼儿园5~6岁儿童近视和近视前期流行特征[J]. 北京大学学报(医学版), 2025, 57(3): 442-447. |
| [5] | 刘光旭, 张良, 赵厚宇, 邓思危, 杨君婷, 李宁, 马瑞, 何艳, 许国章, 刘志科, 詹思延. 2015—2021年宁波市6岁以下儿童热性惊厥的流行病学特征[J]. 北京大学学报(医学版), 2025, 57(3): 584-591. |
| [6] | 李琳, 廖津津. 应用ROC曲线评估久坐行为对儿童青少年视力不良的预测价值[J]. 北京大学学报(医学版), 2025, 57(3): 614-619. |
| [7] | 王紫薇, 李闵, 高慧, 邓芳. 链球菌感染与过敏性紫癜肾炎患儿肾损害的相关性[J]. 北京大学学报(医学版), 2025, 57(2): 284-290. |
| [8] | 邓敏婷, 王楠, 夏斌, 赵玉鸣, 朱俊霞. 儿童及青少年挫入恒前牙自行再萌出的相关影响因素[J]. 北京大学学报(医学版), 2025, 57(1): 148-153. |
| [9] | 杨颖婷, 李若竹, 窦桂丽, 雷玥, 夏斌. iRoot BP Plus用于年轻恒牙外伤部分牙髓切断治疗的临床随机对照研究[J]. 北京大学学报(医学版), 2024, 56(6): 1083-1088. |
| [10] | 赵双云, 邹思雨, 李雪莹, 沈丽娟, 周虹. 中文版口腔健康素养量表简版(HeLD-14)在学龄前儿童家长中应用的信度和效度评价[J]. 北京大学学报(医学版), 2024, 56(5): 828-832. |
| [11] | 陈心心, 唐哲, 乔艳春, 荣文笙. 北京市密云区4岁儿童患龋状况及其与龋活跃性检测的相关性[J]. 北京大学学报(医学版), 2024, 56(5): 833-838. |
| [12] | 岳芷涵,韩娜,鲍筝,吕瑾莨,周天一,计岳龙,王辉,刘珏,王海俊. 儿童早期体重指数轨迹与超重风险关联的前瞻性队列研究[J]. 北京大学学报(医学版), 2024, 56(3): 390-396. |
| [13] | 费秀文,刘斯,汪波,董爱梅. 成人及儿童组织坏死性淋巴结炎临床特征及治疗[J]. 北京大学学报(医学版), 2024, 56(3): 533-540. |
| [14] | 俞光岩. 儿童唾液腺疾病[J]. 北京大学学报(医学版), 2024, 56(1): 1-3. |
| [15] | 闫晓晋,刘云飞,马宁,党佳佳,张京舒,钟盼亮,胡佩瑾,宋逸,马军. 《中国儿童发展纲要(2011-2020年)》实施期间中小学生营养不良率变化及其政策效应分析[J]. 北京大学学报(医学版), 2023, 55(4): 593-599. |
|
||
