北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (1): 35-42. doi: 10.19723/j.issn.1671-167X.2020.01.006
844例牙源性角化囊肿的临床病理学分析
王彦瑾1,谢晓艳2,洪瑛瑛3,白嘉英1,张建运1,△( ),李铁军1,△()
),李铁军1,△()
- 1. 北京大学口腔医学院·口腔医院, 病理科, 北京 100081
2. 北京大学口腔医学院·口腔医院,口腔颌面医学影像科, 北京 100081
3. 北京大学口腔医学院·口腔医院,门诊部 国家口腔疾病临床医学研究中心 口腔数字化医疗技术和材料国家工程实验室 口腔数字医学北京市重点实验室,北京 100081
Clinicopathological analysis of 844 cases of odontogenic keratocysts
Yan-jin WANG1,Xiao-yan XIE2,Ying-ying HONG3,Jia-ying BAI1,Jian-yun ZHANG1,△(),Tie-jun LI1,△()
- 1. Peking University School and Hospital of Stomatology & Department of Oral Pathology, Beijing 100081, China
2. Peking University School and Hospital of Stomatology & Department of Oral and Maxillofacial Radiology, Beijing 100081, China
3. First Clinical Division, Peking University School and Hospital of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
摘要:
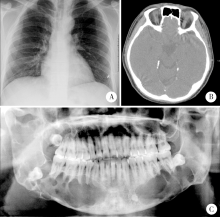
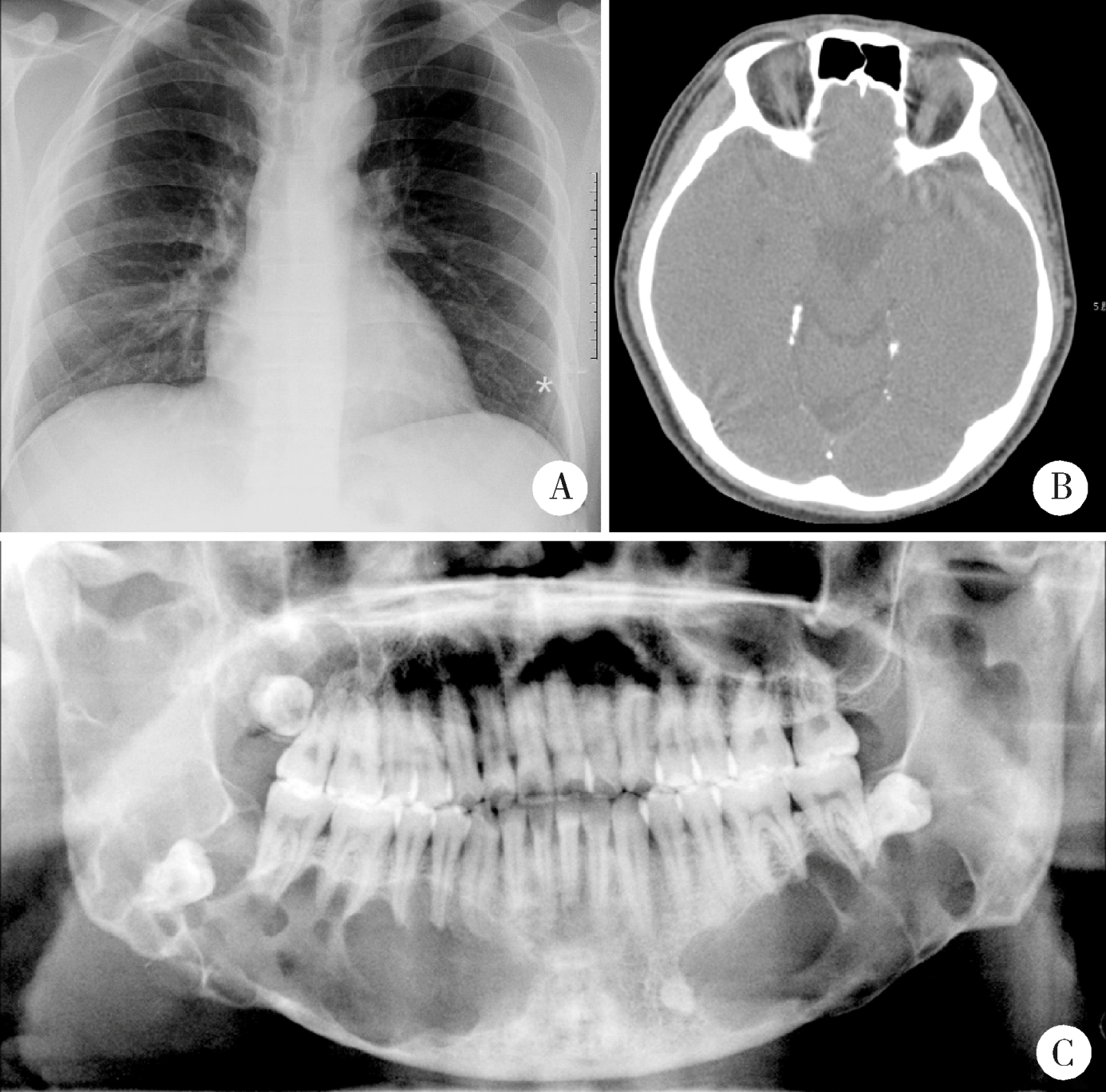
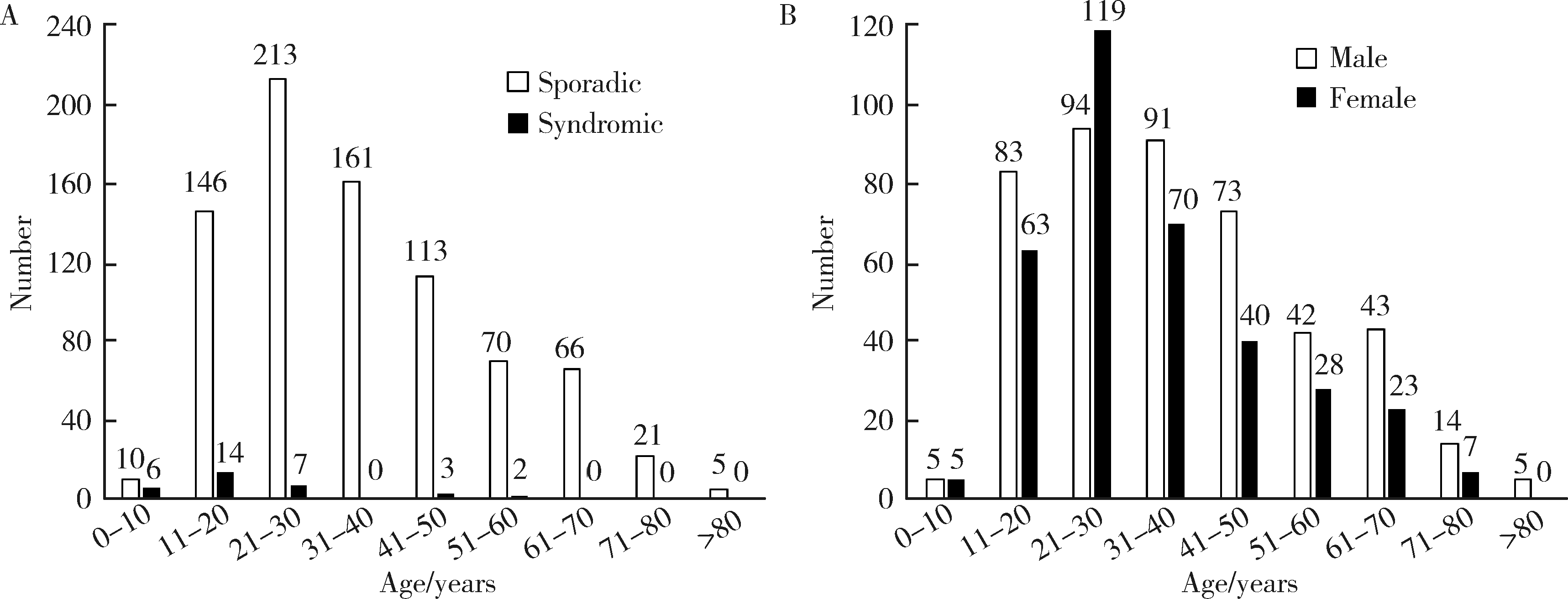
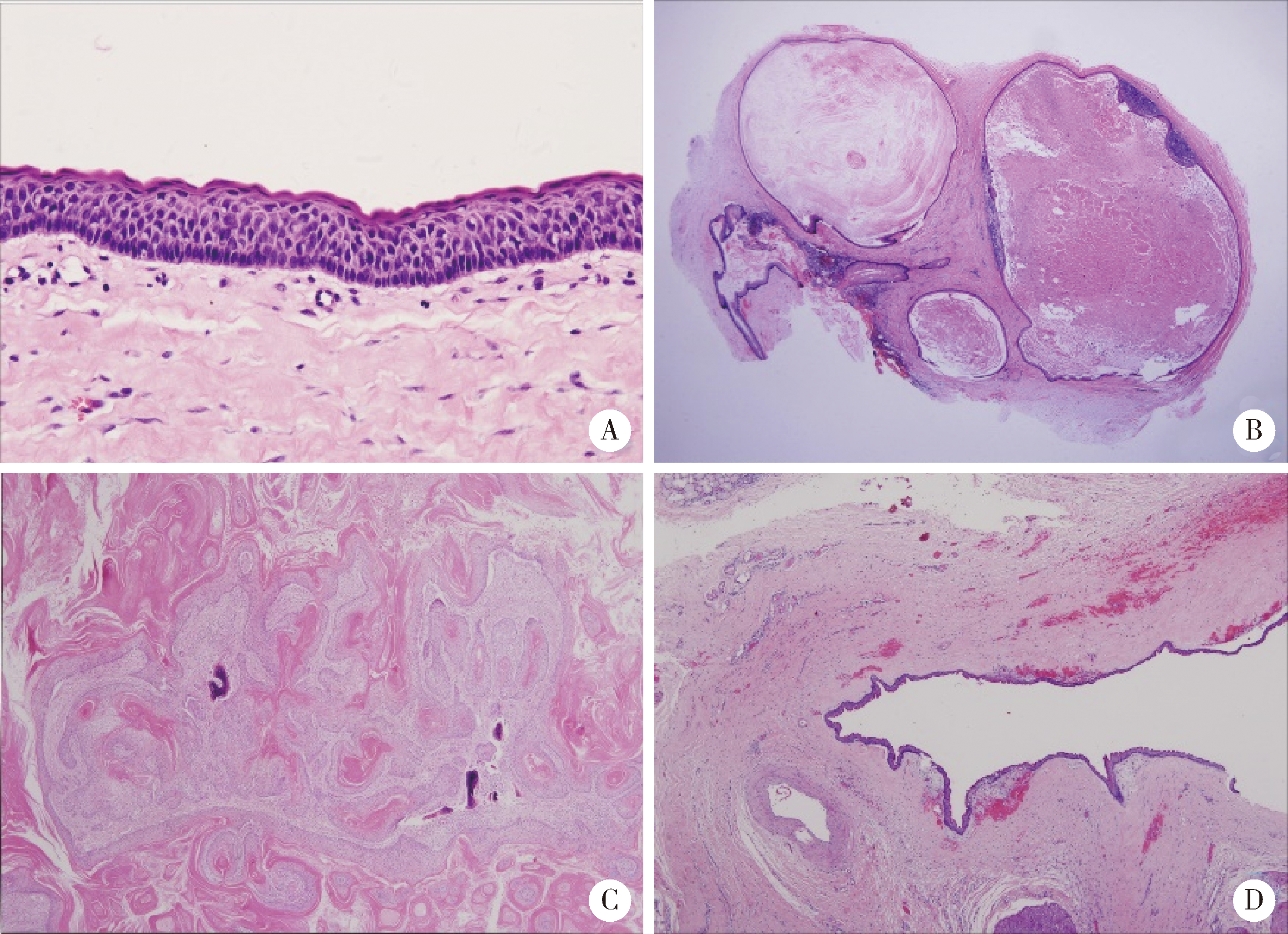
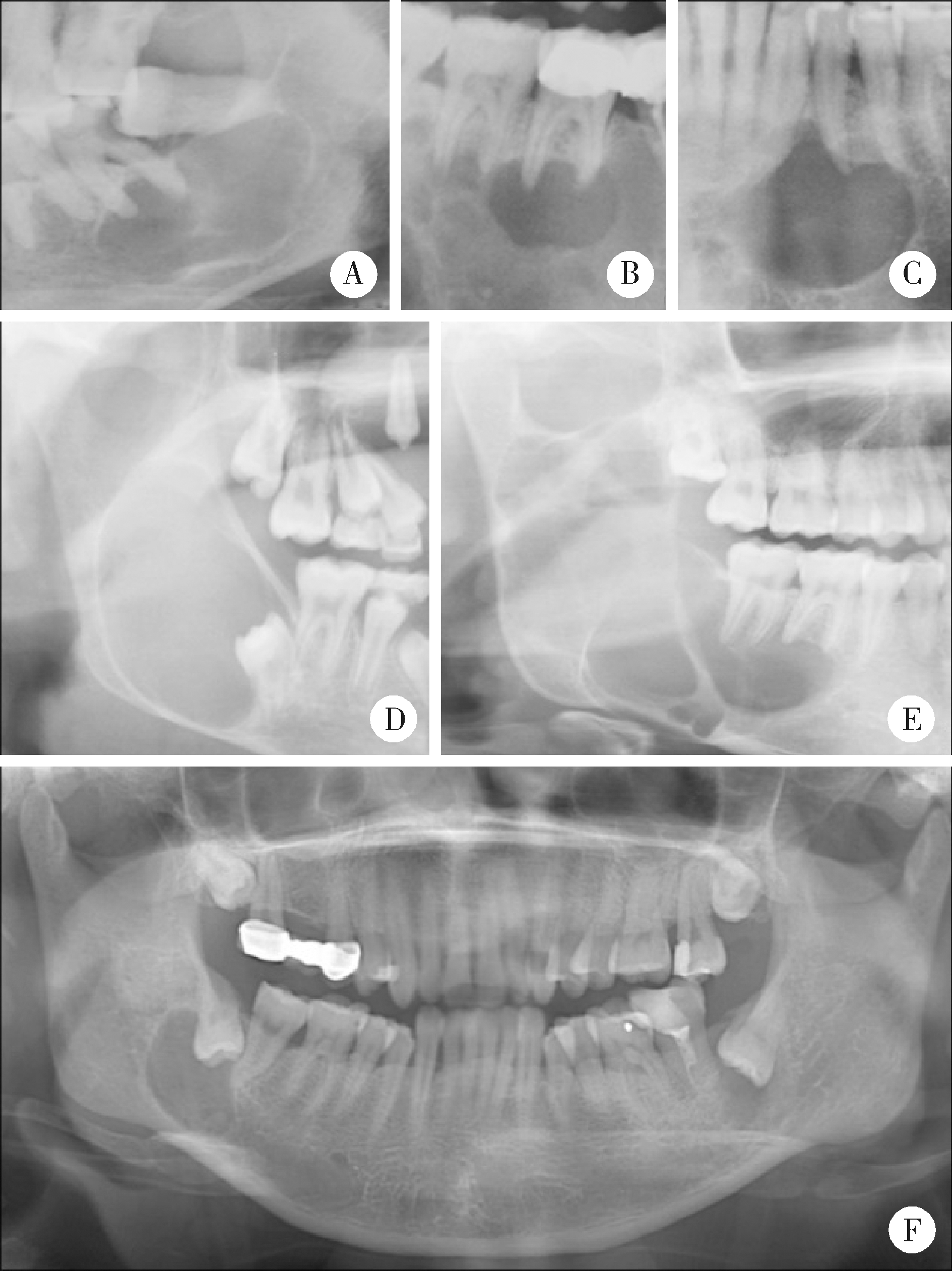
目的:分析牙源性角化囊肿(odontogenic keratocyst, OKC)的临床病理特点及预后相关因素,为临床诊治及预后判断提供依据。方法:收集2000—2018年北京大学口腔医院病理诊断为OKC或与其相关疾病的病例844例,分析其临床资料、影像学及病理特点,分别归类为散发型OKC[发生于颌骨内,不伴痣样基底细胞癌综合征(nevoid basal cell carcinoma syndrome, NBCCS)]、综合征相关OKC、实性型OKC以及外周型OKC四组,并分析患者的治疗及随访资料。结果:844例患者中,散发型OKC患者805例(95.4%),综合征相关OKC患者32例(3.8%),实性型OKC患者3例,外周型OKC患者4例。散发型OKC患者平均年龄36.03岁(11~30岁为发病高峰),男女性别比1.27 ∶1,好发于下颌磨牙升支部(56.2%),经影像学检查,其中428例(71.2%)为单房性病损,多房性病损占28.8%。588例散发型OKC患者行刮治术后有随访资料,其中118例复发(20.1%),复发高峰发生于术后1~3年,影像学呈多房表现者易复发(39.0%),开窗术后刮治术(43例)和单纯刮治术(545例)这两种保守治疗的复发率差异无统计学意义(P>0.05)。综合征相关OKC患者的发病年龄(平均20.97岁)小于散发型OKC,易多发(30/32,93.7%), 好发于下颌磨牙升支部(41.7%),综合征相关OKC组织学上囊壁中含子囊者较散发型OKC多见(分别为56.3%和17.9%),且更易复发(13/29,44.9%)。实性型和外周型OKC患者的年龄较大(平均年龄分别为45.00岁和65.75岁),4例外周型OKC摘除后无复发。结论:散发型OKC行刮治术后的复发率为20.1%,影像学表现多房者更易复发,开窗术后刮治术或单纯刮治术的复发率无明显差异,临床上应注意适应证;综合征相关OKC的发病年龄小、更易多发、刮治后易复发;实性型OKC和外周型OKC少见,患者年龄较大。
中图分类号:
- R739.8




| [1] | El-Naggar A, Chan J, Grandis JR , et al. WHO classification of head and neck tumors[M]. 4th ed. Lyon, France: IARC, 2017: 235-236. |
| [2] | Stoelinga PJW . Keratocystic odontogenic tumour (KCOT) has again been renamed odontogenic keratocyst (OKC)[J]. Int J Oral Maxillofac Surg, 2019,48(3):415-416. |
| [3] | Li TJ . The odontogenic keratocyst: a cyst, or a cystic neoplasm?[J]. J Dent Res, 2011,90(2):133-142. |
| [4] | Bresler SC, Padwa BL, Granter SR . Nevoid basal cell carcinoma syndrome (Gorlin syndrome)[J]. Head Neck Pathol, 2016,10(2):119-124. |
| [5] | Jawa DS, Sircar K, Somani R , et al. Gorlin-Goltz syndrome[J]. J Oral Maxillofac Pathol, 2009,13(2):89-92. |
| [6] | Kawano K, Okamura K, Kashima K , et al. Solid variant of keratocystic odontogenic tumor of the mandible: report of a case with a clear cell component and review of the literature[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2013,116(5):e393-398. |
| [7] | Chi AC, Owings JR Jr, Muller S . Peripheral odontogenic keratocyst: report of two cases and review of the literature[J]. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2005,99(1):71-78. |
| [8] | Luo HY, Li TJ . Odontogenic tumors: a study of 1309 cases in a Chinese population[J]. Oral Oncol, 2009,45(8):706-711. |
| [9] | Gorlin RJ . Nevoid basal cell carcinoma syndrome[J]. Dermatol Clin, 1995,13(1):113-125. |
| [10] | Slusarenko da Silva Y, Stoelinga PJW, Naclério-Homem MDG . Recurrence of nonsyndromic odontogenic keratocyst after marsu-pialization and delayed enucleation vs. enucleation alone: a systematic review and meta-analysis[J]. Oral Maxillofac Surg, 2019,23(1):1-11. |
| [11] | Fidele NB, Yueyu Z, Zhao Y , et al. Recurrence of odontogenic keratocysts and possible prognostic factors: Review of 455 patients[J]. Med Oral Patol Oral Cir Bucal, 2019,24(4):e491-e501. |
| [12] | Stoelinga PJ . Long-term follow-up on keratocysts treated according to a defined protocol[J]. Int J Oral Maxillofac Surg, 2001,30(1):14-25. |
| [13] | Cunha JF, Gomes CC, de Mesquita RA , et al. Clinicopathologic features associated with recurrence of the odontogenic keratocyst: a cohort retrospective analysis[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2016,121(6):629-635. |
| [14] | 李铁军 . 牙源性角化囊肿的生长与行为[J]. 中华口腔医学杂志, 2000, ( 04):66-68. |
| [15] | Sigua-Rodriguez EA, Goulart DR, Sverzut A , et al. Is surgical treatment based on a 1-step or 2-step protocol effective in managing the odontogenic keratocyst? [J]. J Oral Maxillofac Surg, 2019, 77(6): 1210. e1-1210. e7. |
| [16] | 陶谦, 兰天俊 . 开窗治疗颌骨囊性病变的临床思考与循证[J]. 口腔疾病防治, 2018,26(12):759-765. |
| [17] | Al-Moraissi EA, Dahan AA, Alwadeai MS , et al. What surgical treatment has the lowest recurrence rate following the management of keratocystic odontogenic tumor?: A large systematic review and meta-analysis[J]. J Craniomaxillofac Surg, 2017,45(1):131-144. |
| [18] | Vazquez-Romero MD, Serrera-Figallo ML, Alberdi-Navarro J , et al. Maxillary peripheral keratocystic odontogenic tumor. A clinical case report[J]. J Clin Exp Dent, 2017,9(1):e167-e171. |
| [1] | 欧俊永,倪坤明,马潞林,王国良,颜野,杨斌,李庚午,宋昊东,陆敏,叶剑飞,张树栋. 肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素[J]. 北京大学学报(医学版), 2024, 56(4): 582-588. |
| [2] | 刘帅,刘磊,刘茁,张帆,马潞林,田晓军,侯小飞,王国良,赵磊,张树栋. 伴静脉癌栓的肾上腺皮质癌的临床治疗及预后[J]. 北京大学学报(医学版), 2024, 56(4): 624-630. |
| [3] | 虞乐,邓绍晖,张帆,颜野,叶剑飞,张树栋. 具有低度恶性潜能的多房囊性肾肿瘤的临床病理特征及预后[J]. 北京大学学报(医学版), 2024, 56(4): 661-666. |
| [4] | 周泽臻,邓绍晖,颜野,张帆,郝一昌,葛力源,张洪宪,王国良,张树栋. 非转移性T3a肾细胞癌患者3年肿瘤特异性生存期预测[J]. 北京大学学报(医学版), 2024, 56(4): 673-679. |
| [5] | 方杨毅,李强,黄志高,陆敏,洪锴,张树栋. 睾丸鞘膜高分化乳头状间皮肿瘤1例[J]. 北京大学学报(医学版), 2024, 56(4): 741-744. |
| [6] | 曾媛媛,谢云,陈道南,王瑞兰. 脓毒症患者发生正常甲状腺性病态综合征的相关因素[J]. 北京大学学报(医学版), 2024, 56(3): 526-532. |
| [7] | 苏俊琪,王晓颖,孙志强. 舌鳞状细胞癌根治性切除术后患者预后预测列线图的构建与验证[J]. 北京大学学报(医学版), 2024, 56(1): 120-130. |
| [8] | 李建斌,吕梦娜,池强,彭一琳,刘鹏程,吴锐. 干燥综合征患者发生重症新型冠状病毒肺炎的早期预测[J]. 北京大学学报(医学版), 2023, 55(6): 1007-1012. |
| [9] | 刘欢锐,彭祥,李森林,苟欣. 基于HER-2相关基因构建风险模型用于膀胱癌生存预后评估[J]. 北京大学学报(医学版), 2023, 55(5): 793-801. |
| [10] | 薛子璇,唐世英,邱敏,刘承,田晓军,陆敏,董靖晗,马潞林,张树栋. 青年肾肿瘤伴瘤栓的临床病理特征及预后分析[J]. 北京大学学报(医学版), 2023, 55(5): 802-811. |
| [11] | 卢汉,张建运,杨榕,徐乐,李庆祥,郭玉兴,郭传瑸. 下颌牙龈鳞状细胞癌患者预后的影响因素[J]. 北京大学学报(医学版), 2023, 55(4): 702-707. |
| [12] | 时云飞,王豪杰,刘卫平,米岚,龙孟平,刘雁飞,赖玉梅,周立新,刁新婷,李向红. 血管免疫母细胞性T细胞淋巴瘤临床与分子病理学特征分析[J]. 北京大学学报(医学版), 2023, 55(3): 521-529. |
| [13] | 朱晓娟,张虹,张爽,李东,李鑫,徐玲,李挺. 人表皮生长因子受体2低表达乳腺癌的临床病理学特征及预后[J]. 北京大学学报(医学版), 2023, 55(2): 243-253. |
| [14] | 赖玉梅,李忠武,李欢,吴艳,时云飞,周立新,楼雨彤,崔传亮. 68例肛管直肠黏膜黑色素瘤临床病理特征及预后[J]. 北京大学学报(医学版), 2023, 55(2): 262-269. |
| [15] | 沈棋,刘亿骁,何群. 肾黏液样小管状和梭形细胞癌的临床病理特点及预后[J]. 北京大学学报(医学版), 2023, 55(2): 276-282. |
|
||
