北京大学学报(医学版) ›› 2026, Vol. 58 ›› Issue (3): 650-657. doi: 10.19723/j.issn.1671-167X.2026.03.027
544例慢性唾液腺炎的临床与影像学特点及病因分析
杨静, 许晓韵, 郑丹妮, 凌晓彤, 屈留洋, 柳登高*( )
)
- 北京大学口腔医学院·口腔医院医学影像科,国家口腔医学中心,国家口腔疾病临床医学研究中心,口腔生物材料和数字诊疗装备国家工程研究中心,口腔数字医学北京市重点实验室,国家卫生健康委员会口腔医学计算机应用工程技术研究中心,国家药品监督管理局口腔生物材料重点实验室,北京 100081
Clinical and imaging characteristics and etiology of 544 cases with chronic sialadenitis
Jing YANG, Xiaoyun XU, Danni ZHENG, Xiaotong LING, Liuyang QU, Denggao LIU*()
- Department of Oral and Maxillofacial Radiology, Peking University School and Hospital of Stomatology & National Center for Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Research Center of Oral Biomaterials and Digital Medical Devices & Beijing Key Laboratory of Digital Stomatology & NHC Research Center of Engineering and Technology for Computerized Dentistry & NMPA Key Laboratory for Dental Materials, Beijing 100081, China
摘要:
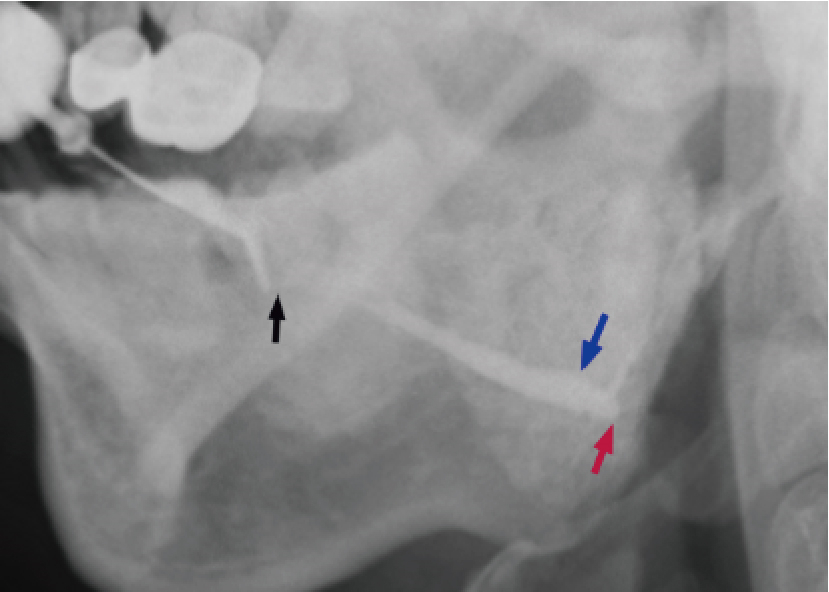
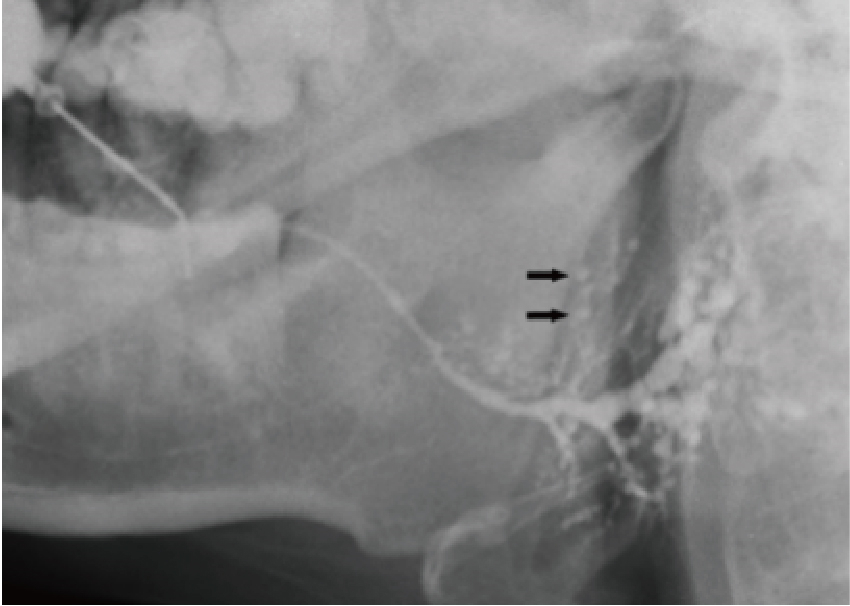
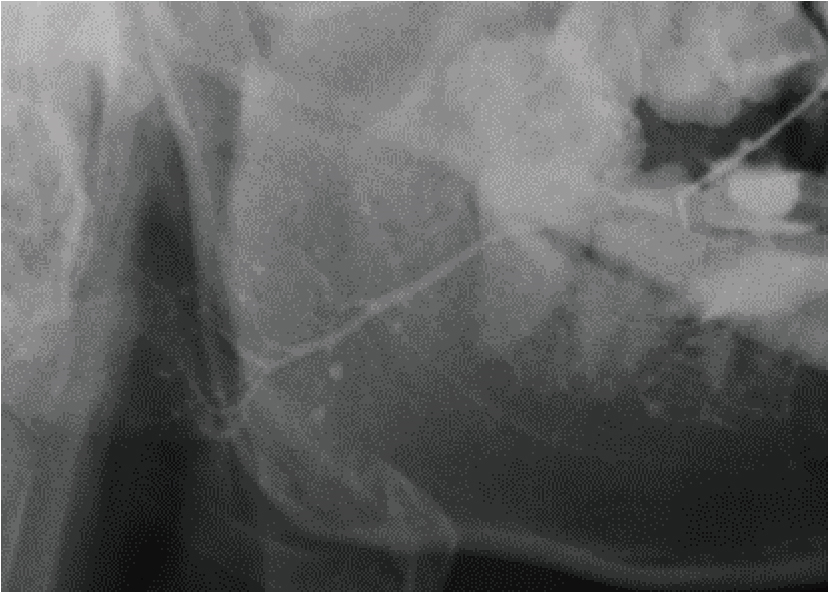
目的: 探索临床上常见的几类不同病因导致的慢性唾液腺炎的占比,并分析其临床和影像学特点。方法: 回顾性分析2021年1月至2023年8月就诊于北京大学口腔医院并行唾液腺内镜治疗的各类慢性唾液腺炎患者的临床及影像资料,除外干燥综合征伴感染、IgG4相关唾液腺炎、结石病伴感染等,根据现有研究结果和资料,初步将唾液腺炎分为131I相关唾液腺炎、过敏相关唾液腺炎、成人复发性腮腺炎、腮腺良性肥大伴管炎、原发性导管狭窄性唾液腺炎(指未发现目前已知的可能病因,并存在导管狭窄的慢性唾液腺炎),统计分析各类慢性唾液腺炎的占比和主要临床、影像学特点。结果: 共纳入544例患者,男性192例、女性352例,平均年龄(47.44±13.52)岁(14~83岁)。其中,原发性导管狭窄性唾液腺炎最多,占71.7%(390例);过敏相关唾液腺炎次之,占12.5%(68例);131I相关唾液腺炎占6.4%(35例),成人复发性腮腺炎占4.8%(26例),腮腺良性肥大伴管炎占4.6%(25例)。544例患者共1 120侧腺体受累,包括腮腺880侧(78.6%)及下颌下腺240侧(21.4%)。这五类唾液腺炎在性别、年龄、受累腺体类别、受累腺体数目及病程上差异均存在统计学意义(P < 0.05),131I相关唾液腺炎患者的女性占比最高(男∶女=1 ∶ 4.83),成人复发性腮腺炎患者的平均年龄最小[(32.50±8.60)岁],131I相关唾液腺炎和过敏相关唾液腺炎的受累腺体数目相对较多。从造影表现看,131I相关唾液腺炎中23.2%的受累腺体发生导管闭锁,过敏相关唾液腺炎中46.5%的受累腺体分支导管呈“雪花样”扩张表现,成人复发性腮腺炎中80.4%的受累腺体可见末梢导管“点球状扩张”,腮腺良性肥大伴管炎的受累腺体分支导管呈丛簇状表现者占71.4%,原发性导管狭窄性唾液腺炎的造影表现以主导管(主导管和分支导管)狭窄和(或)扩张为主。结论: 原发性导管狭窄性唾液腺炎、131I相关唾液腺炎、过敏相关唾液腺炎、成人复发性腮腺炎、腮腺良性肥大伴管炎是临床上常见的五类慢性唾液腺炎,其中原发性导管狭窄性唾液腺炎占比最大。明确各类慢性唾液腺炎的病因、临床及影像学特征,将有利于临床医师制定个性化治疗方案,改善治疗效果。
中图分类号:
- R781.72



| 1 |
doi: 10.1002/lary.24211 |
| 2 |
doi: 10.1016/j.jormas.2021.05.010 |
| 3 |
doi: 10.1016/j.joms.2014.06.438 |
| 4 |
doi: 10.1007/s00405-023-07834-z |
| 5 |
俞光岩, 柳登高, 李巍, 等. 3类新型慢性唾液腺炎的诊断和治疗[J]. 北京大学学报(医学版), 2022, 54 (1): 13- 17.
doi: 10.19723/j.issn.1671-167X.2022.01.003 |
| 6 |
|
| 7 |
doi: 10.1111/odi.13821 |
| 8 |
doi: 10.1111/odi.12595 |
| 9 |
doi: 10.1097/MD.0000000000005132 |
| 10 |
doi: 10.1002/lary.29508 |
| 11 |
doi: 10.1111/odi.13434 |
| 12 |
doi: 10.1097/MNM.0000000000000325 |
| 13 |
|
| 14 |
doi: 10.1089/105072503321582060 |
| 15 |
doi: 10.1089/thy.2012.0243 |
| 16 |
doi: 10.1002/hed.26417 |
| 17 |
doi: 10.1007/s12149-013-0735-3 |
| 18 |
doi: 10.1016/j.archoralbio.2015.06.003 |
| 19 |
俞光岩, 宿骞, 张艳, 等. 唾液腺疾病与全身系统性疾病的相关性[J]. 北京大学学报(医学版), 2023, 55 (1): 1- 7.
doi: 10.19723/j.issn.1671-167X.2023.01.001 |
| 20 |
doi: 10.1111/odi.12526 |
| 21 |
俞光岩, 洪霞, 李巍, 等. IgG4相关唾液腺炎的临床病理特点及诊断[J]. 北京大学学报(医学版), 2019, 51 (1): 1- 3.
doi: 10.19723/j.issn.1671-167X.2019.01.001 |
| 22 |
doi: 10.1186/s13075-015-0888-7 |
| 23 |
doi: 10.1016/j.jcms.2015.06.036 |
| 24 |
doi: 10.14639/0392-100X-1605 |
| 25 |
doi: 10.1016/j.otc.2021.02.005 |
| 26 |
doi: 10.1016/j.joms.2020.11.032 |
| 27 |
doi: 10.1016/j.bjoms.2012.07.013 |
| 28 |
doi: 10.1007/s00405-019-05445-1 |
| 29 |
doi: 10.14639/0392-100X-1600 |
| 30 |
doi: 10.1177/0194599820957256 |
| 31 |
doi: 10.1016/j.ijporl.2021.110617 |
| 32 |
王松灵, 丁刚. 慢性腮腺炎性疾病的诊断与治疗[J]. 中国实用口腔科杂志, 2008, 1 (3): 132- 135.
|
| 33 |
doi: 10.1016/j.joms.2003.08.041 |
| 34 |
doi: 10.1089/thy.2016.0266 |
| 35 |
doi: 10.1089/thy.2019.0563 |
| 36 |
doi: 10.1007/s00405-022-07473-w |
| 37 |
doi: 10.1016/j.oooo.2020.05.015 |
| 38 |
俞光岩. 涎腺疾病[M]. 北京: 北京医科大学、中国协和医科大学联合出版社, 1994: 77- 78.
|
| [1] | 丛馨, 苏家增, 吴立玲, 丁冲, 李巍, 俞光岩. 唾液腺非肿瘤性疾病诊治研究进展[J]. 北京大学学报(医学版), 2026, 58(1): 1-9. |
| [2] | 杨雨婷, 屈留洋, 郑丹妮, 凌晓彤, 许晓韵, 柳登高. 1 812例唾液腺结石患者的人口学特征和临床特点[J]. 北京大学学报(医学版), 2026, 58(1): 153-159. |
| [3] | 杨源源, 张珊珊, 俞光岩, 杨辉俊, 杨宏宇. 部分下颌下腺切除术治疗下颌下腺良性肿瘤的临床效果[J]. 北京大学学报(医学版), 2025, 57(2): 334-339. |
| [4] | 杨玉淑, 齐晅, 丁萌, 王炜, 郭惠芳, 高丽霞. 抗唾液腺蛋白1抗体联合抗腮腺分泌蛋白抗体对干燥综合征的诊断价值[J]. 北京大学学报(医学版), 2024, 56(5): 845-852. |
| [5] | 俞光岩. 儿童唾液腺疾病[J]. 北京大学学报(医学版), 2024, 56(1): 1-3. |
| [6] | 柳登高,郑丹妮,赵雅宁,张亚琼,叶欣,张丽琪,谢晓艳,张雷,张祖燕,俞光岩. 疑难唾液腺结石病的治疗研究[J]. 北京大学学报(医学版), 2023, 55(1): 8-12. |
| [7] | 俞光岩,苏家增,柳登高,吴立玲,丛馨. 下颌下腺保存治疗新技术体系的建立与应用[J]. 北京大学学报(医学版), 2022, 54(5): 842-845. |
| [8] | 李炳雨,唐祖南,胡耒豪,章文博,于尧,俞光岩,彭歆. 腮腺微小肿瘤的临床病理研究[J]. 北京大学学报(医学版), 2022, 54(2): 335-339. |
| [9] | 俞光岩,柳登高,李巍,洪霞,张严妍,朱文瑄,张可夫,李潇,栗占国,刘燕鹰,陈艳,高岩,苏家增. 3类新型慢性唾液腺炎的诊断和治疗[J]. 北京大学学报(医学版), 2022, 54(1): 13-17. |
| [10] | 陈超伦,苏家增,俞光岩. 酸刺激对腮腺和下颌下腺唾液流率及成分的影响[J]. 北京大学学报(医学版), 2022, 54(1): 89-94. |
| [11] | 朱忆颖,闵赛南,俞光岩. 局部注射环孢素A对非肥胖糖尿病小鼠下颌下腺分泌功能及炎症的影响[J]. 北京大学学报(医学版), 2021, 53(4): 750-757. |
| [12] | 俞光岩. 多发性唾液腺肿大的鉴别诊断及处理[J]. 北京大学学报(医学版), 2021, 53(1): 1-4. |
| [13] | 王怡平,蔡志刚,彭歆,张杰,孙志鹏,李巍,张雷,俞光岩. 下颌下腺质量和体积的实体体外检测[J]. 北京大学学报(医学版), 2021, 53(1): 126-132. |
| [14] | 李潇,苏家增,张严妍,张丽琪,张亚琼,柳登高,俞光岩. 131I相关唾液腺炎的炎症分级及内镜治疗[J]. 北京大学学报(医学版), 2020, 52(3): 586-590. |
| [15] | 李玉冰,孙丽莎,孙志鹏,谢晓艳,张建运,张祖燕,赵燕平,马绪臣. 腮腺CT影像报告与数据系统的初步研究[J]. 北京大学学报(医学版), 2020, 52(1): 83-89. |
|
||
