北京大学学报(医学版) ›› 2019, Vol. 51 ›› Issue (4): 684-688. doi: 10.19723/j.issn.1671-167X.2019.04.015
肾上腺区巨大肿瘤合并瘤栓的诊断与治疗
刘磊1,王国良1,马潞林1,△( ),陆敏2,刘承1,侯小飞1
),陆敏2,刘承1,侯小飞1
- 1. 北京大学第三医院 泌尿外科, 北京 100191
2. 北京大学第三医院 病理科, 北京 100191
Diagnosis and surgical treatment of massive adrenal area tumor with tumor thrombus
Lei LIU1,Guo-liang WANG1,Lu-lin MA1,△(),Min LU2,Cheng LIU1,Xiao-fei HOU1
- 1. Department of Urology, Peking University Third Hospital, Beijing 100191, China
2. Department of Pathology, Peking University Third Hospital, Beijing 100191, China
摘要:
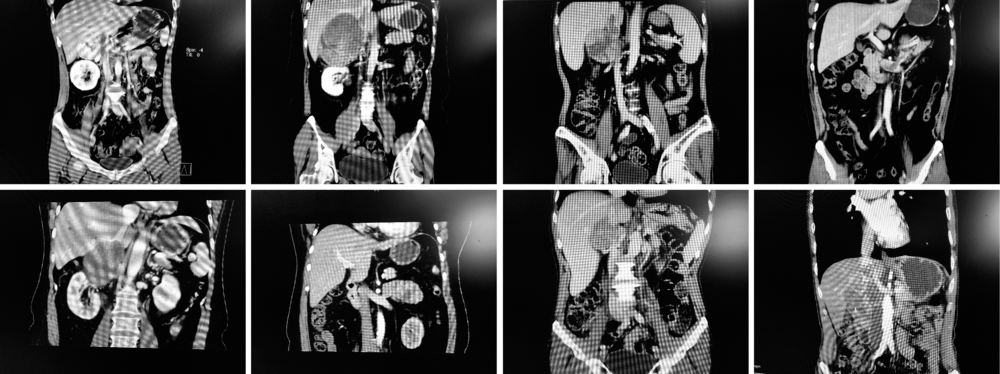
目的:总结临床上少见的肾上腺区巨大肿瘤合并静脉瘤栓的诊断和手术经验。方法:自2017年10月至2019年3月,共8例肾上腺区巨大肿瘤(>7cm)合并静脉瘤栓病例就诊于北京大学第三医院,包括男性5例、女性3例,平均年龄50.6岁(31~62岁),右侧6例、左侧2例。首发症状包括腹部不适、高血压、Cushing面容、月经异常;特殊既往史包括肝硬化、肺癌。所有病例行影像学和内分泌学检查,术前影像学已明确合并下腔静脉瘤栓5例、左肾静脉瘤栓1例;术中发现合并肾上腺中央静脉瘤栓2例。4例右侧合并下腔静脉瘤栓且瘤栓上极较高病例实施开放肿瘤切除及瘤栓切除术,3例行腹腔镜手术(右侧2例、左侧1例),1例未行手术治疗。结果:平均肿瘤大小8.9 cm(7~11 cm),平均手术时间319 min(120~510 min),平均出血量629 mL(50~1 200 mL),术中输血2例,伤口感染1例。肿瘤类型:嗜铬细胞瘤1例、肾上腺皮质癌3例、肾上腺转移瘤2例、肾上腺区平滑肌肉瘤2例。术中发现嗜铬细胞瘤瘤栓中混合机化血栓;肾上腺皮质癌层次欠清,包膜极易破;肾上腺转移瘤血供丰富;肾上腺区平滑肌肉瘤均侵犯下腔静脉形成瘤栓,血供不丰富。平均随访时间8.4个月(1~15个月),1例肾上腺皮质癌术后4个月发生肝转移,于1年后死亡。结论:合并瘤栓的肾上腺区巨大肿瘤种类多,术前诊断有一定难度,需全面评估和完善术前准备;其手术难度大,方式多样,开放手术以及腹腔镜手术均可行。
中图分类号:
- R736.6

| [1] | Gaujoux S, Weinandt M, Bonnet S , et al. Surgical treatment of adrenal carcinoma[J]. J Visc Surg, 2017,154(5):335-343. |
| [2] | Chiche L, Dousset B, Kieffer E , et al. Adrenocortical carcinoma extending into the inferior vena cava: Presentation of a 15-patient series and review of the literature[J]. Surgery, 2006,139(1):15-27. |
| [3] | Ayala-Ramirez M, Jasim S, Feng L , et al. Adrenocortical carcinoma: clinical outcomes and prognosis of 330 patients at a tertiary care center[J]. Eur J Endocrinol, 2013,169(6):891-899. |
| [4] | Wang Y, Zhou F, Pan H , et al. Adrenal cortical carcinoma with tumor thrombus extension into the right atrium: A case report[J]. Oncol Lett, 2016,11(6):3987-3991. |
| [5] | Fassnacht M, Libé R, Kroiss M , et al. Adrenocortical carcinoma: a clinician’s update[J]. Nat Rev Endocrinol. 2011,7(6):323-335. |
| [6] | Tritos NA, Cushing GW, Heatley G , et al. Clinical features and prognostic factors associated with adrenocortical carcinoma: Lahey Clinic Medical Center experience[J]. Am Surg, 2000,66(1):73-79. |
| [7] | Chen Y, Chomsky-Higgins K, Nwaogu I , et al. Trends in adrenal surgery: The changing nature of tumors and patients[J]. J Surg Res, 2019,236(4):129-133. |
| [8] | Kota SK, Kota SK, Jammula S , et al. Pheochromocytoma with inferior vena cava thrombosis: An unusual association[J]. Cardiovasc Dis Res, 2012,3(2):160-164. |
| [9] | Amr F. Adrenal masses: A urological perspective [J]. Arab J Urol, 2016, 26, 14(4):248-255. |
| [10] | Dull BZ, Smith B, Tefera G , et al. Surgical management of retroperitoneal leiomyosarcoma arising from the inferiorvena cava[J]. J Gastrointest Sur, 2013,17(12):2166-2171. |
| [11] | Lenders JW, Eisenhofer G, Mannelli M , et al. Phaeochromocytoma[J]. Lancet, 2005,366(9486):655-675. |
| [12] | 刘茁, 马潞林, 田晓军 , 等. 肾癌根治性切除加癌栓取出术治疗Mayo Ⅲ级下腔静脉癌栓的手术技术及临床经验[J]. 北京大学学报(医学版), 2017,49(4):597-602. |
| [13] | Baudin E, Pellegriti G, Bonnay M , et al. Impact of monitoring plasma 1,1-dichlorodiphenildichloroethane (o,p’DDD) levels on the treatment of patients with adrenocortical carcinoma[J]. Can-cer, 2001,92(6):1385-1392. |
| [1] | 马豆豆, 马晓彩, 常天静, 王丽芳, 丁艳, 石连杰. 临床表现似系统性红斑狼疮的大B细胞淋巴瘤骨髓受累1例[J]. 北京大学学报(医学版), 2026, 58(3): 666-669. |
| [2] | FarinEbrahimi, 冯志强, FarazEbrahimi, 韩玮华, 于子杨, 贾宽宽, 安金刚. 上颌药物相关性颌骨坏死的不同分期手术治疗效果[J]. 北京大学学报(医学版), 2026, 58(1): 107-114. |
| [3] | 赵业, 刁小莉, 熊焰. 细胞转移技术在微量细胞液病理诊断中的应用[J]. 北京大学学报(医学版), 2026, 58(1): 208-213. |
| [4] | 王月, 梁宇红. 繁茂型牙骨质-骨结构不良1例[J]. 北京大学学报(医学版), 2026, 58(1): 220-224. |
| [5] | 池彦廷, 蒋鸿杰, 陈艳, 徐志秀, 李斌斌. 直接免疫荧光在口腔黏膜寻常型天疱疮诊断中的价值: 基于多指标联合分析的回顾性研究[J]. 北京大学学报(医学版), 2026, 58(1): 68-73. |
| [6] | 顾静妍, 李欣艺, 赵金霞, 穆荣. 误诊为类风湿关节炎、痛风的糖尿病致Charcot关节病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1193-1197. |
| [7] | 王晓林, 李璐瑶, 张雯, 王鸿雁. 3例子宫体中肾样腺癌的临床病理学分析[J]. 北京大学学报(医学版), 2025, 57(6): 1208-1212. |
| [8] | 王小梦, 曾晓君, 李娟. 黎族与汉族系统性红斑狼疮患者的主要临床特征[J]. 北京大学学报(医学版), 2025, 57(6): 1213-1218. |
| [9] | 肖晓笛, 夏有辰, 柳剑英, 付鹏. 左侧胸锁乳突肌间血管内乳头状内皮增生1例[J]. 北京大学学报(医学版), 2025, 57(5): 1002-1004. |
| [10] | 孙翔宇, 袁超, 周芯竹, 刁婧, 郑树国. 唾液微生态在口腔及全身疾病早期防治中的应用[J]. 北京大学学报(医学版), 2025, 57(5): 859-863. |
| [11] | 刘帅, 刘茁, 管允鹤, 王国良, 田晓军, 张洪宪, 刘磊, 马潞林, 张树栋. 机器人辅助腹腔镜下腔静脉节段性切除术治疗肾肿瘤瘤栓侵犯血管壁[J]. 北京大学学报(医学版), 2025, 57(4): 796-802. |
| [12] | 孙建军, 马千权, 尹晓亮, 杨辰龙, 张嘉, 陈素华, 吴超, 谢京城, 韩芸峰, 林国中, 司雨, 杨军, 邬海博, 赵强. 任意维度重建磁共振对骶管囊肿进行精准分型对于指导微创手术和康复的意义[J]. 北京大学学报(医学版), 2025, 57(2): 303-308. |
| [13] | 陈钊, 邱永康, 康磊. 经典型Sweet综合征 18F-FDG PET/CT多脏器异常显像1例[J]. 北京大学学报(医学版), 2025, 57(2): 403-407. |
| [14] | 方媛媛, 徐帆, 雷杰, 张昊, 张文宇, 孙宇, 吴宏新, 傅开元, 毛伟玉. 基于颞下颌关节紊乱病诊断标准的临床自动诊断系统的建立及验证[J]. 北京大学学报(医学版), 2025, 57(1): 192-201. |
| [15] | 王红彦, 李鑫铭, 房柯池, 朱华群, 贾汝琳, 王晶. 系统性红斑狼疮疾病活动度相关特征分析及评估模型的构建[J]. 北京大学学报(医学版), 2024, 56(6): 1017-1022. |
|
||
