北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (3): 470-478. doi: 10.19723/j.issn.1671-167X.2020.03.012
孕早期血清维生素E水平与妊娠期高血压疾病发病风险的关系
孟文颖1,黄琬桐2,张杰2,焦明远3,金蕾4,靳蕾2,△( )
)
- 1. 北京市通州区妇幼保健院产科,北京 101100
2. 北京大学生育健康研究所,国家卫生健康委员会生育健康重点实验室,北京大学公共卫生学院流行病与卫生统计学系,北京 100191
3. 北京市通州区妇幼保健院检验科,北京 101100
4. 北京市通州区妇幼保健院妇女保健科,北京 101100
Relationship between serum vitamin E concentration in first trimester and the risk of developing hypertension disorders complicating pregnancy
Wen-ying MENG1,Wan-tong HUANG2,Jie ZHANG2,Ming-yuan JIAO3,Lei JIN4,Lei JIN2,△()
- 1. Department of Obstetrics, Tongzhou Maternal & Child Health Hospital of Beijing, Beijing 101100, China
2. Institute of Reproductive and Child Health, National Health Commission Key Laboratory of Reproductive Health, Peking University, Beijing 100191, China; Department of Epidemiology and Biostatistics, Peking University School of Public Health, Beijing 100191, China
3. Department of Clinical Laboratory, Tongzhou Maternal & Child Health Hospital of Beijing, Beijing 101100, China
4. Department of Maternal Health Care, Tongzhou Maternal & Child Health Hospital of Beijing, Beijing 101100, China
摘要:
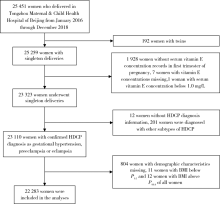
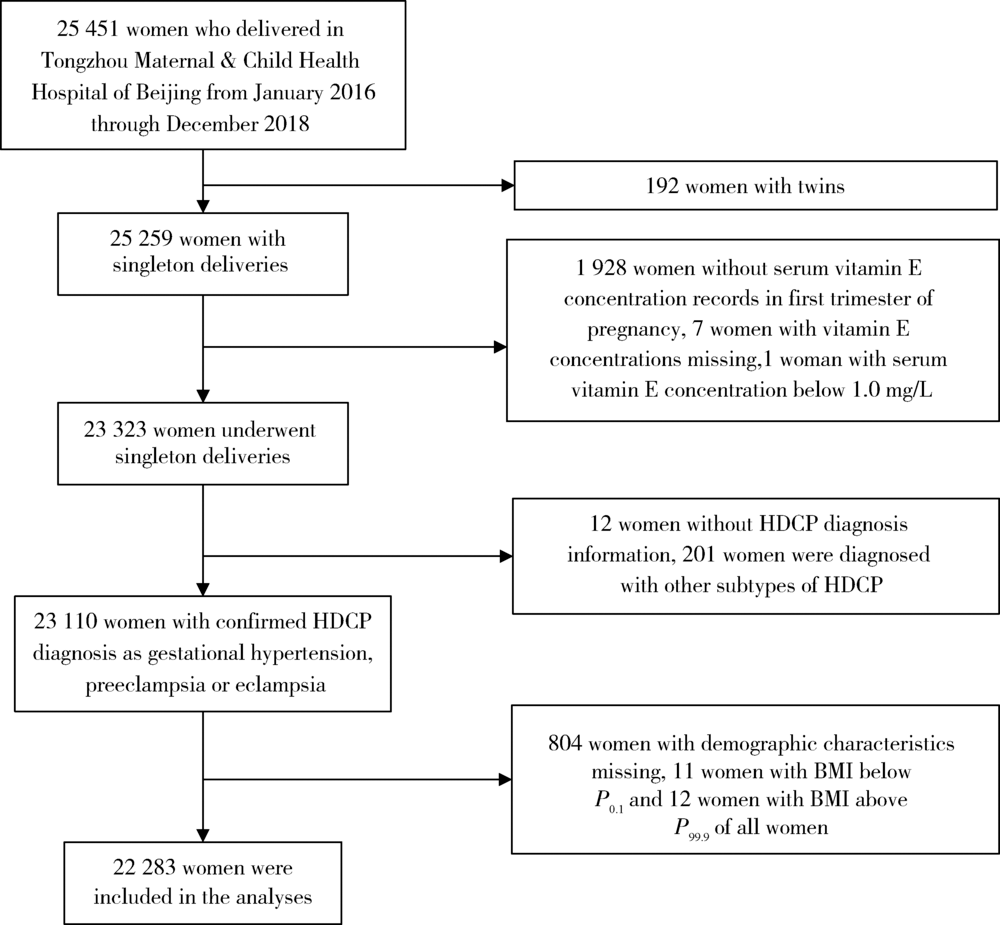
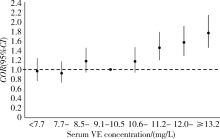
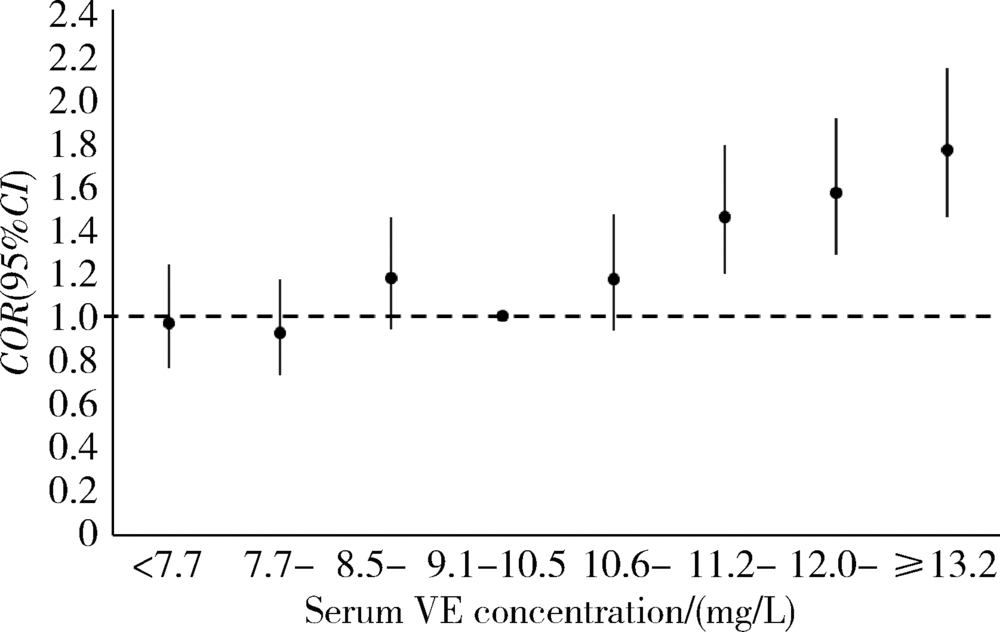
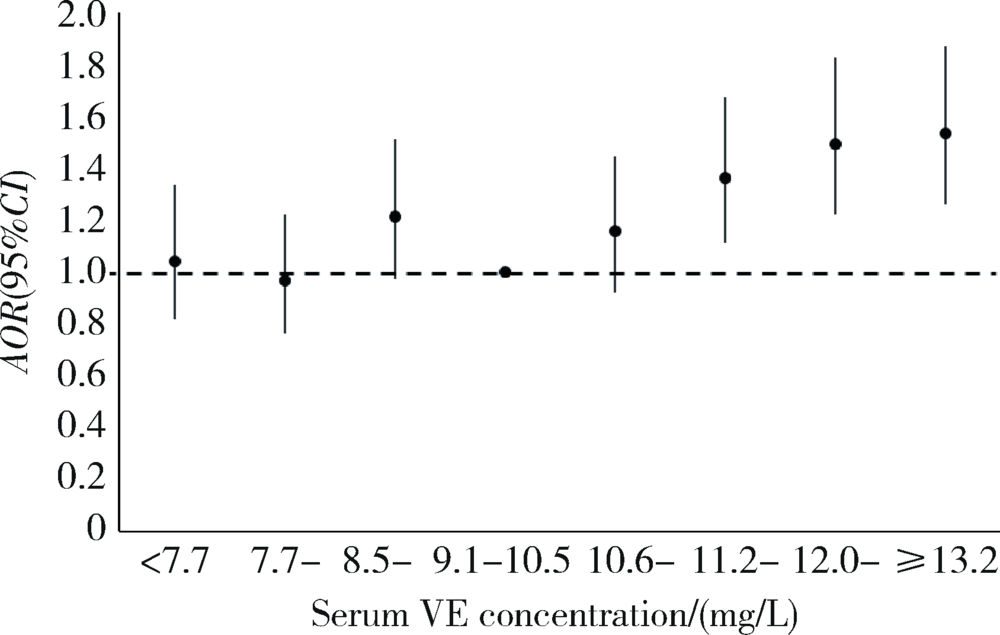
目的 了解北京妇女妊娠期高血压疾病(hypertension disorders complicating pregnancy, HDCP)发病率和孕早期维生素E(vitamin E, VE)营养状况,探究孕早期血清VE浓度与HDCP发病率的关系。方法 以北京市通州区孕期保健系统和通州区妇幼保健院医院信息系统为基础,利用2016年1月至 2018年12月在北京市通州区妇幼保健院分娩并在孕早期测定了血清VE浓度的22 283名单胎孕产妇的信息进行回顾性队列研究,用非条件Logistic回归模型分析不同血清VE浓度与HDCP发病风险的关系。结果 HDCP总发病率为5.4%,其中妊娠期高血压发病率为2.1%,子痫前期-子痫发病率为3.3%。妇女孕早期血清VE浓度中位值为10.1(8.8 ~ 11.6) mg/L,99.7%的妇女孕早期血清VE水平处于正常参考值范围内。3年间,妇女孕早期血清VE浓度(P < 0.001)及HDCP的发病率(P = 0.005)均有逐年上升趋势。单因素与多因素Logistic回归分析结果显示,血清VE浓度较高的孕妇HDCP的发病风险更高;在多因素Logistic回归分析中,与血清VE浓度在百分位数
中图分类号:
- R172
| [1] | 谢幸, 苟文丽. 妇产科学[M]. 8版. 北京: 人民卫生出版社, 2013: 42, 64. |
| [2] | 中华医学会妇产科学分会妊娠期高血压疾病学组. 妊娠期高血压疾病诊治指南(2015)[J]. 中华围产医学杂志, 2016,19(3):161-169. |
| [3] |
Umesawa M, Kobashi G. Epidemiology of hypertensive disorders in pregnancy: prevalence, risk factors, predictors and prognosis[J]. Hypertens Res, 2017,40(3):213-220.
pmid: 27682655 |
| [4] | Ye C, Ruan Y, Zou L, et al. The 2011 survey on hypertensive disorders of pregnancy (HDP) in China: prevalence, risk factors, complications, pregnancy and perinatal outcomes[J]. PLoS One, 2014,9(6):e100180. |
| [5] |
You SH, Cheng PJ, Chung TT, et al. Population-based trends and risk factors of early- and late-onset preeclampsia in Taiwan 2001—2014[J]. BMC Pregnancy Childbirth, 2018,18(1):199.
pmid: 29855344 |
| [6] | Paré E, Parry S, McElrath TF, et al. Clinical risk factors for preeclampsia in the 21st century[J]. Obstet Gynecol, 2014,124(4):763-770. |
| [7] |
Redman CW, Sargent IL. Latest advances in understanding preeclampsia[J]. Science, 2005,308(5728):1592-1594.
pmid: 15947178 |
| [8] | 殷为, 钟梅. 妊娠期高血压疾病的病因、预测及诊疗进展[J]. 实用医学杂志, 2016,32(11):1887-1890. |
| [9] | 孙长颢. 营养与食品卫生学[M]. 8版. 北京: 人民卫生出版社, 2017: 93-95, 215. |
| [10] | 郭方, 李笑天. 叶酸及多种维生素的补充对妊娠期高血压疾病的预防作用[J]. 中国实用妇科与产科杂志, 2014,30(8):592-596. |
| [11] | Rumbold A, Ota E, Hori H, et al. Vitamin E supplementation in pregnancy[J]. Cochrane Database Syst Rev, 2015(9): CD004069. |
| [12] |
Zhang C, Williams MA, Sanchez SE, et al. Plasma concentrations of carotenoids, retinol, and tocopherols in preeclamptic and normotensive pregnant women[J]. Am J Epidemiol, 2001,153(6):572-580.
pmid: 11257065 |
| [13] | Roberts JM, Myatt L, Spong CY, et al. Vitamins C and E to prevent complications of pregnancy-associated hypertension[J]. N Engl J Med, 2010,362(14):1282-1291. |
| [14] | Poston L, Briley AL, Seed PT, et al. Vitamin C and vitamin E in pregnant women at risk for pre-eclampsia (VIP trial): randomised placebo-controlled trial[J]. Lancet, 2006,367(9517):1145-1154. |
| [15] |
Rajasingam D, Seed PT, Briley AL, et al. A prospective study of pregnancy outcome and biomarkers of oxidative stress in nulliparous obese women[J]. Am J Obstet Gynecol, 2009,200(4):395.
pmid: 19200933 |
| [16] | 康忠春, 陈远兰, 邹余粮. 妊娠子痫前期孕妇维生素A、E水平及其影响因素分析[J]. 临床医学研究与实践, 2018,3(30):142-144. |
| [17] | 张翠, 靳颖, 杨洁, 等. 河北省产妇2016年妊娠期高血压疾病患病情况分析[J]. 中国公共卫生, 2018,34(10):1395-1397. |
| [18] | 牛影, 徐叶清, 郝加虎, 等. 马鞍山市妇女孕前体质指数和孕期增重与妊娠期高血压疾病的队列研究[J]. 卫生研究, 2016,45(2):205-210. |
| [19] | 申南, 陆娣, 郑春梅, 等. 常规保健下不同年龄段孕妇妊娠早期血清维生素A、E水平分析[J]. 中国妇产科临床杂志, 2018,19(4):356-358. |
| [20] | 闫明, 张雯, 刘凯波, 等. 北京地区2010年—2017年增补叶酸预防神经管缺陷工作效果分析[J]. 中国优生与遗传杂志, 2019,27(3):339-341. |
| [21] | Schiff E, Friedman SA, Stampfer M, et al. Dietary consumption and plasma concentrations of vitamin E in pregnancies complicated by preeclampsia[J]. Am J Obstet Gynecol, 1996,175(4 Pt 1):1024-1028. |
| [22] |
Bartsch E, Medcalf KE, Park AL, et al. Clinical risk factors for pre-eclampsia determined in early pregnancy: systematic review and meta-analysis of large cohort studies[J]. BMJ, 2016,353:i1753.
pmid: 27094586 |
| [23] | Rumbold AR, Crowther CA, Haslam RR, et al. Vitamins C and E and the risks of preeclampsia and perinatal complications[J]. N Engl J Med, 2006,354(17):1796-1806. |
| [24] | Bowman BA, Russell RM. 现代营养学[M]. 8版. 荫士安,汪之顼, 译. 北京: 化学工业出版社, 2004: 195. |
| [25] | Karpińska J, Mikołuć B, Motkowski R, et al. HPLC method for simultaneous determination of retinol, alpha-tocopherol and coenzyme Q10 in human plasma [J]. J Pharm Biomed Anal, 2006,42(2):232-236. |
| [26] | 马蕊, 刘建蒙, 李松, 等. 浙江省嘉兴地区妊娠高血压综合征发病状况研究[J]. 中华流行病学杂志, 2005,26(12):960-963. |
| [27] | Yusuf H, Subih HS, Obeidat BS, et al. Associations of macro and micronutrients and antioxidants intakes with preeclampsia: A case-control study in Jordanian pregnant women[J]. Nutr Metab Car-diovasc Dis, 2019,29(5):458-466. |
| [28] | 孟凡文, 陈森, 刘亚山, 等. 河北省5县区妊娠期高血压疾病的发病情况及危险因素分析[J]. 中国生育健康杂志, 2015,26(2):112-115. |
| [1] | 王玉霖, 郜鑫, 刘志科, 詹思延. 2018—2023年江苏省0~3岁婴幼儿肠套叠发病的流行病学特征[J]. 北京大学学报(医学版), 2026, 58(3): 490-495. |
| [2] | 徐慧颖, 何兴侯, 黄薇, 张彬, 李梦瑶, 刘家辉, 方言, 赵二璐, 魏相睿, 马旭, 杨英. 中国育龄女性围孕期冷热暴露与先天性心脏病发病风险的关联[J]. 北京大学学报(医学版), 2026, 58(3): 503-512. |
| [3] | 陆梦溪, 王炳翰, 康佳丽, 刘秋萍, 周逸帆, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 生物学年龄在社区人群队列中预测心血管病风险的应用[J]. 北京大学学报(医学版), 2026, 58(3): 543-550. |
| [4] | 李欣艺, 赵金霞, 穆荣. 阿司匹林对系统性红斑狼疮妊娠者结局的影响[J]. 北京大学学报(医学版), 2025, 57(6): 1074-1080. |
| [5] | 范梦, 王梦莹, 王斯悦, 彭和香, 王雪珩, 郭煌达, 侯天姣, 秦雪英, 陈大方, 胡永华, 李劲, 武轶群, 吴涛. 动脉硬化相关指标与死亡风险的前瞻性队列研究[J]. 北京大学学报(医学版), 2025, 57(6): 1153-1159. |
| [6] | 陆梦溪, 刘秋萍, 周恬静, 刘晓非, 孙烨祥, 沈鹏, 林鸿波, 唐迅, 高培. 基于社区人群队列的甘油三酯-葡萄糖指数与心血管病发病和死亡的关联[J]. 北京大学学报(医学版), 2025, 57(3): 430-435. |
| [7] | 杨树涵, 李奕昕, 崔浩亮, 王佑新, 吴玉莹, 王明月, 杨依凡, 恩卡尔·努尔, 杨磊, 王辉. 代谢相关脂肪性肝病及其心脏代谢风险指标异常与不良妊娠结局的相关性[J]. 北京大学学报(医学版), 2025, 57(3): 487-495. |
| [8] | 卞雯, 周文君, 吴天晨, 朱培静, 陈一诺, 原鹏波, 王学举, 王颖, 魏瑗, 赵扬玉. 单绒毛膜双羊膜囊双胎妊娠双胎之一胎死宫内对妊娠结局的影响[J]. 北京大学学报(医学版), 2025, 57(3): 592-598. |
| [9] | 王文琼, 侯玉珂, 李春, 张学武. 系统性红斑狼疮患者不良妊娠结局的预测因素[J]. 北京大学学报(医学版), 2025, 57(3): 599-603. |
| [10] | 杨俊娟, 张蕾, 张龑. 妊娠合并脐尿管瘘1例[J]. 北京大学学报(医学版), 2025, 57(2): 393-395. |
| [11] | 谢芳菲, 乔虹, 李博雅, 袁翠, 王芳, 孙瑜, 李双玲. 妊娠期重度营养不良合并急性肾盂肾炎致脓毒症、难治性感染性休克、多器官功能衰竭1例[J]. 北京大学学报(医学版), 2025, 57(1): 202-207. |
| [12] | 王明霞, 丁菱, 王敏, 邹婵娟, 颜丝语, 梁颖文, 王伟佳, 何善智. 双靶点嵌合抗原受体T细胞治疗系统性红斑狼疮患者停药后安全孕产1例[J]. 北京大学学报(医学版), 2024, 56(6): 1119-1125. |
| [13] | 马会超,李军,王永清. 妊娠合并炎症性肠病的临床特点[J]. 北京大学学报(医学版), 2024, 56(2): 260-266. |
| [14] | 李洋洋,侯林,马紫君,黄山雅美,刘捷,曾超美,秦炯. 孕期因素与婴儿牛奶蛋白过敏的关系[J]. 北京大学学报(医学版), 2024, 56(1): 144-149. |
| [15] | 刘晓强,周寅. 牙种植同期植骨术围术期高血压的相关危险因素[J]. 北京大学学报(医学版), 2024, 56(1): 93-98. |
|
||
