北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (2): 353-361. doi: 10.19723/j.issn.1671-167X.2020.02.025
结直肠间质瘤临床病理特征及预后分析
王文鹏1,王捷夫1,胡均1,王俊锋1,刘嘉1,孔大陆1,△( ),李健2
),李健2
- 1. 大连医科大学附属第一医院放射科, 辽宁大连 116011
2. 北京大学医学部医学技术研究院, 北京 100191
Clinicopathological features and prognosis of colorectal stromal tumor
Wen-peng WANG1,Jie-fu WANG1,Jun HU1,Jun-feng WANG1,Jia LIU1,Da-lu KONG1,△(),Jian LI2
- 1. Department of Radiology, the First Affiliated Hospital of Dalian Medical University, Dalian 116011, Liaoning, China
2. Institute of Medical Technology, Peking University Health Science Center, Beijing 100191, China
摘要:
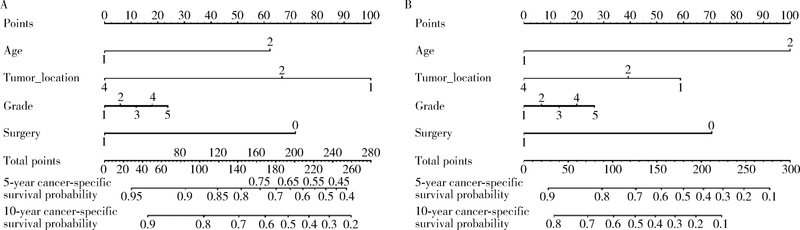
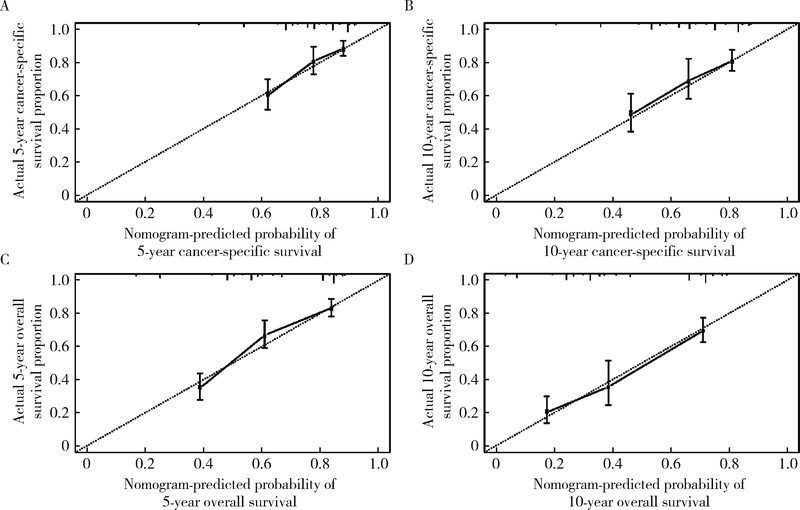
目的 探究结直肠间质瘤预后相关因素,并通过列线图预测该肿瘤生存概率,为指导临床评估预后提供依据.方法: 通过监测流行病学和最终结果(surveillance, epidemiology, and end results, SEER)数据库获取1992年1月至2015年12月结直肠间质瘤临床病理及预后相关资料,对入组患者进行生存分析,将分析得到的独立预后因素绘制成列线图,之后采用校准曲线评估列线图预测生存准确性.结果: 546例结直肠间质瘤患者被纳入研究.中位发病年龄64岁,区域淋巴结转移率9.4%.546例患者多因素生存分析显示发病年龄 > 64岁,未婚/离婚,结肠间质瘤(与直肠间质瘤相比),非手术治疗,组织分化级别高,区域淋巴结转移及远处转移具有更差的肿瘤特异性生存和总生存(P均<0.05), 美国东部地区诊治患者比西部地区患者具有更长的总生存时间(P = 0.027),以上独立预后因素预测肿瘤特异性生存率和总生存率的C指数分别为0.76(95%CI: 0.72-0.80)和0.75(95%CI: 0.72-0.78).在174例组织分化级别和肿瘤部位明确的患者中,影响肿瘤特异性生存和总生存的独立预后因素为年龄,组织分化级别和是否行手术治疗(P均<0.05),而肿瘤部位仅与肿瘤特异性生存显著相关(P = 0.041),未证实与总生存显著相关(P = 0.057),采用这4个预后影响因素预测546例患者肿瘤特异性生存率和总生存率的C指数分别是0.71(95%CI: 0.66-0.75)和0.73(95%CI: 0.70-0.77), 能较准确预测结直肠间质瘤患者总生存率.结论: 结直肠间质瘤预后受多个临床病理因素影响,列线图能为预测结直肠间质瘤患者生存率提供依据.
中图分类号:
- R735.3

| [1] | Nilsson B, Bumming P, Meis-Kindblom JM , et al. Gastrointestinal stromal tumors: the incidence, prevalence, clinical course, and prognostication in the preimatinib mesylate era: a population-based study in western Sweden[J]. Cancer, 2005,103(4):821-829. |
| [2] | Parab TM , DeRogatis MJ, Boaz AM, et al. Gastrointestinal stromal tumors: a comprehensive review[J]. J Gastrointest Oncol, 2019,10(1):144-154. |
| [3] | Kindblom LG, Remotti HE, Aldenborg F , et al. Gastrointestinal pacemaker cell tumor (GIPACT): gastrointestinal stromal tumors show phenotypic characteristics of the interstitial cells of Cajal[J]. Am J Pathol, 1998,152(5):1259-1269. |
| [4] | Soreide K, Sandvik OM, Soreide JA , et al. Global epidemiology of gastrointestinal stromal tumours (GIST): A systematic review of population-based cohort studies[J]. Cancer Epidemiol, 2016,40:39-46. |
| [5] | Corbin KS, Kindler HL, Liauw SL . Considering the role of radiation therapy for gastrointestinal stromal tumor[J]. Onco Targets Ther, 2014,7:713-718. |
| [6] | Wu PC, Langerman A, Ryan CW , et al. Surgical treatment of gastrointestinal stromal tumors in the imatinib (STI-571) era[J]. Surgery, 2003,134(4):656-665. |
| [7] | 杨朝纲, 熊斌 . 结直肠间质瘤诊治进展[J]. 实用癌症杂志, 2015,30(10):1575-1577. |
| [8] | Miettinen M, Lasota J, Sobin LH . Gastrointestinal stromal tumors of the stomach: A clinicopathologic, immunohistochemical, and molecular genetic study of 1 765 cases with longterm follow-up[J]. Am J Surg Pathol, 2005,29(10):1373-1381. |
| [9] | Al-Thani H, El-Menyar A, Rasul KI , et al. Clinical presentation, management and outcomes of gastrointestinal stromal tumors[J]. Int J Surg, 2014,12(10):1127-1133. |
| [10] | Cao H, Zhang Y, Wang M , et al. Prognostic analysis of patients with gastrointestinal stromal tumors: a single unit experience with surgical treatment of primary disease[J]. Chin Med J (Engl), 2010,123(2):131-136. |
| [11] | Varshney VK, Gupta RK, Saluja SS , et al. Analysis of clinicopathological and immunohistochemical parameters and correlation of outcomes in gastrointestinal stromal tumors[J]. Indian J Can-cer, 2019,56(2):135-143. |
| [12] | Ghanem N, Altehoefer C, Furtwangler A , et al. Computed tomography in gastrointestinal stromal tumors[J]. Eur Radiol, 2003,13(7):1669-1678. |
| [13] | Tateishi U, Hasegawa T, Satake M , et al. Gastrointestinal stromal tumor. Correlation of computed tomography findings with tumor grade and mortality[J]. J Comput Assist Tomogr, 2003,27(5):792-798. |
| [14] | Gaitanidis A, El Lakis M, Alevizakos M , et al. Predictors of lymph node metastasis in patients with gastrointestinal stromal tumors (GISTs)[J]. Langenbecks Arch Surg, 2018,403(5):599-606. |
| [15] | Tokunaga M, Ohyama S, Hiki N , et al. Incidence and prognostic value of lymph node metastasis on c-Kit-positive gastrointestinal stromal tumors of the stomach[J]. Hepatogastroenterology, 2011,58(109):1224-1228. |
| [16] | Zhu R, Liu F, Grisotti G , et al. Distinctive features of gastrointestinal stromal tumors arising from the colon and rectum[J]. J Gastrointest Oncol, 2018,9(2):231-240. |
| [17] | 黄湘辉, 裘科跃, 袁旦平 , 等. 102例胃肠间质瘤外科手术疗效及预后影响因素分析[J]. 解放军医学院学报, 2019,40(7):655-659. |
| [18] | Ge XY, Lei LW, Ge F , et al. Analysis of risk factors of gastrointestinal stromal tumors in different age groups based on SEER database[J]. Scand J Gastroenterol, 2019,54(4):480-484. |
| [19] | Buja A, Lago L, Lago S , et al. Marital status and stage of cancer at diagnosis: A systematic review[J]. Eur J Cancer Care (Engl), 2018,27 (2017-08-29)[2019-10-30]. |
| [20] | Li J, Ye Y, Wang J , et al. Chinese consensus guidelines for diagnosis and management of gastrointestinal stromal tumor[J]. Chinese Journal of Cancer Research, 2017,29(4):281-293. |
| [21] | Wada R, Arai H, Kure S , et al. "Wild type" GIST: Clinicopathological features and clinical practice[J]. Pathol Int, 2016,66(8):431-437. |
| [22] | 艾力·赛丁, 艾克拜尔·艾力, 张成 , 等. DOG1在胃肠道间质瘤中的表达及其临床意义[J]. 现代肿瘤医学, 2016,24(21):3418-3421. |
| [23] | 李超亿, 梁小波, 马俊杰 , 等. C-kit与血小板源性生长因子受体基因突变特征与胃肠间质瘤患者预后的关系[J]. 中华胃肠外科杂志, 2012,15(3):271-275. |
| [1] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [2] | 舒帆, 葛力源, 邓汉彰, 殷昊明, 欧俊永, 邓绍晖, 郝一昌, 陆敏, 张展奕, 段佩辰, 张树栋. 预后不良的肾细胞癌伴淋巴结转移的分子特征[J]. 北京大学学报(医学版), 2026, 58(3): 631-640. |
| [3] | 王楠楠, 袁大晋, 朱昱冰, 丁磊. 结直肠癌根治术后肝转移风险多中心列线图预测模型的构建与验证[J]. 北京大学学报(医学版), 2026, 58(2): 290-300. |
| [4] | 张铃福, 陈明, 赵小宇, 王港, 崔龙, 凌晓锋, 王立新, 徐智, 郭丽梅, 侯纯升. 原发灶局限于胆囊壁内胆囊癌大体分型及其与预后和癌前病变的相关性[J]. 北京大学学报(医学版), 2026, 58(1): 184-189. |
| [5] | 高雅静, 李正芳, 马梦思, 武丽君. SII和SIRI对白塞病葡萄膜炎的风险预测及疾病活动度和预后的评估[J]. 北京大学学报(医学版), 2025, 57(6): 1067-1073. |
| [6] | 李博闻, 张强, 孙益鑫. 儿童及青年漏斗胸患者Nuss术后发生脊柱侧弯的风险预测模型建立及验证[J]. 北京大学学报(医学版), 2025, 57(5): 941-946. |
| [7] | 郭博达, 陆敏, 王国良, 张洪宪, 刘磊, 侯小飞, 赵磊, 田晓军, 张树栋. 肾透明细胞癌与非透明细胞癌伴静脉癌栓患者的临床病理特征及预后比较[J]. 北京大学学报(医学版), 2025, 57(4): 644-649. |
| [8] | 李伟浩, 李晶, 张学民, 李伟, 李清乐, 张小明. 术中回收式自体输血对颈动脉体瘤切除术后肿瘤预后的影响[J]. 北京大学学报(医学版), 2025, 57(2): 272-276. |
| [9] | 毛雅晴, 陈震, 于尧, 章文博, 刘洋, 彭歆. 2型糖尿病对口腔鳞状细胞癌患者预后的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1089-1096. |
| [10] | 罗丹, 黄海建, 陈新, 陈小岩. 原发子宫肝样腺癌2例临床病理分析及文献复习[J]. 北京大学学报(医学版), 2024, 56(6): 1126-1131. |
| [11] | 刘园梅, 傅义程, 郝靖欣, 张福春, 刘慧琳. 老年髋部骨折患者住院期间发生术后心力衰竭的列线图预测模型的构建及验证[J]. 北京大学学报(医学版), 2024, 56(5): 874-883. |
| [12] | 李志存, 吴天俣, 梁磊, 范宇, 孟一森, 张骞. 穿刺活检单针阳性前列腺癌术后病理升级的危险因素分析及列线图模型构建[J]. 北京大学学报(医学版), 2024, 56(5): 896-901. |
| [13] | 欧俊永,倪坤明,马潞林,王国良,颜野,杨斌,李庚午,宋昊东,陆敏,叶剑飞,张树栋. 肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素[J]. 北京大学学报(医学版), 2024, 56(4): 582-588. |
| [14] | 刘帅,刘磊,刘茁,张帆,马潞林,田晓军,侯小飞,王国良,赵磊,张树栋. 伴静脉癌栓的肾上腺皮质癌的临床治疗及预后[J]. 北京大学学报(医学版), 2024, 56(4): 624-630. |
| [15] | 虞乐,邓绍晖,张帆,颜野,叶剑飞,张树栋. 具有低度恶性潜能的多房囊性肾肿瘤的临床病理特征及预后[J]. 北京大学学报(医学版), 2024, 56(4): 661-666. |
|
||
