北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (2): 261-265. doi: 10.19723/j.issn.1671-167X.2021.02.005
影响双能CT尿酸盐结晶检出率的因素
谢一帆,王昱,邓雪蓉,耿研,季兰岚,张卓莉( )
)
- 北京大学第一医院风湿免疫科, 北京 100034
Analysis of risk factors influencing the detection rate of urate crystal by dual energy computed tomography
XIE Yi-fan,WANG Yu,DENG Xue-rong,GENG Yan,JI Lan-lan,ZHANG Zhuo-li()
- Department of Rheumatology and Clinical Immunology,Peking University First Hospital, Beijing 100034, China
摘要:
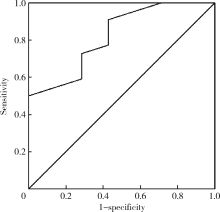
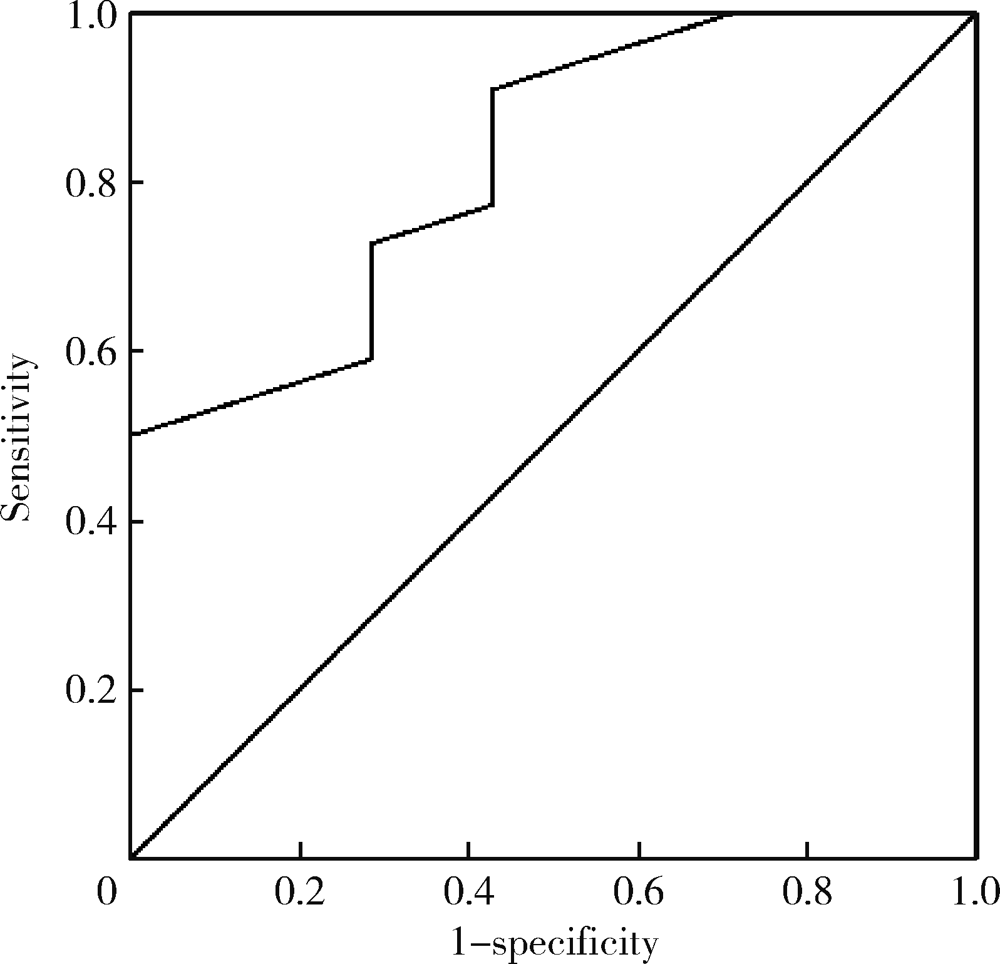
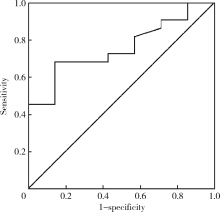
目的: 探讨金标准明确诊断的痛风患者中双能CT(dual energy computed tomography, DECT)检出尿酸盐结晶的影响因素。方法: 选择2011年6月至2018年12月,在北京大学第一医院门诊或住院患者关节滑液偏振光分析尿酸晶体阳性诊断为急性或慢性痛风的病例资料进行回顾性分析,所有患者均接受关节液或痛风石分析和DECT扫描。采用卡方检验、二元Logistics回归及t检验,分析DECT结果与临床资料、实验室检查及药物治疗的关系。结果: 共29例患者入组本研究,22例DECT检出尿酸盐结晶,7例未检出,根据是否检出尿酸盐晶体分为两组,与DECT阴性组相比较,DECT阳性组年龄更高[(47±12)岁vs.(39±11)岁,P=0.15], 体重指数(body bass index,BMI)更高[(27.9±3.7) kg/m2vs.(22.8±2.1) kg/m2,P=0.002],痛风病程更长[(135±102)个月vs.(45±53)个月, P=0.035];阳性组既往血尿酸最高值亦高于DECT阴性组[(643±121) μmol/L vs.(543±103) μmol/L,P=0.043];阳性组患者DECT时血清尿酸值虽然高于DECT阴性组[(558±150) μmol/L vs.(513±88.9) μmol/L,P=0.497], 但差异无统计学意义;DECT检查阳性组与阴性组相比较,检查时处于急性期的患者分别为18例(81.8%) vs.4例(57%), P=0.311;服用降尿酸药物的患者分别为22例(100%) vs.5例(71%), P=0.052;反复典型发作的患者分别为22例(100%) vs.6例(85%), P=0.241。各关节症状与DECT发现尿酸盐结晶一致性比较,右膝关节最高(Kappa=0.627), 其后依次为左第一跖趾(metatarsophalangeal 1, MTP1, Kappa=0.58)、右MTP1(Kappa=0.551)、左膝(Kappa=0.494),均具统计学意义,踝关节症一致性较低(右踝:Kappa=0.19,左踝:Kappa=0.256),均无统计学意义。与DECT尿酸盐晶体检出率有关的变量分别为BMI[2.307(1.139~4.670) kg/m2, P=0.02]、痛风病程 [ 0.306(0.906~4.881)年,P=0.186]、既往尿酸最高值 [0.023(0.981~2.764) mg/dL, P=0.137]。结论: BMI较大、既往最高尿酸值较高、痛风病程较长的痛风患者DECT检出的敏感性越高。
中图分类号:
- R589.7

| [1] |
Roddy E, Choi HK. Epidemiology of gout[J]. Rheum Dis Clin North Am, 2014,40(2):155-175.
pmid: 24703341 |
| [2] | 邓雪蓉, 王昱, 张卓莉. 新型影像学技术在痛风诊治中的应用进展[J]. 中国实用内科杂志, 2018,38(12):1119-1122. |
| [3] | Wang Y, Deng X, Xu Y, et al. Detection of uric acid crystal deposition by ultrasonography and dual-energy computed tomography: A cross-sectional study in patients with clinically diagnosed gout[J]. Medicine (Baltimore), 2018,97(42):e12834. |
| [4] |
Ogdie A, Taylor WJ, Weatherall M, et al. Imaging modalities for the classification of gout: systematic literature review and meta-analysis[J]. Ann Rheum Dis, 2015,74(10):1868-1874.
pmid: 24915980 |
| [5] |
Choi HK, Burns LC, Shojania K, et al. Dual energy CT in gout: a prospective validation study[J]. Ann Rheum Dis, 2012,71(9):1466-1471.
pmid: 22387729 |
| [6] |
Sun C, Qi X, Tian Y, et al. Risk factors for the formation of double-contour sign and tophi in gout[J]. J Orthop Surg Res, 2019,14(1):239.
pmid: 31358044 |
| [7] |
Loeb JN. The influence of temperature on the solubility of monosodium urate[J]. Arthritis Rheum, 1972,15(2):189-192.
pmid: 5027604 |
| [8] |
Horvath SM, Hollander JL. Intra-articular temperature as a measure of joint reaction[J]. J Clin Invest, 1949,28(3):469-473.
pmid: 16695699 |
| [9] | Fiddis RW, VlachosL N, Calvert PD. Studies of urate crystallisation in relation to gout[J]. Ann Rheum Dis, 1983,42(Suppl 1):5-12. |
| [10] |
Tak HK, Cooper SM, Wilcox WR. Studies on the nucleation of monosodium urate at 37 degrees c[J]. Arthritis Rheum, 1980,23(5):574-580.
pmid: 7378087 |
| [11] |
Perez-Ruiz F, Calabozo M, Pijoan JI, et al. Effect of urate-lowering therapy on the velocity of size reduction of tophi in chronic gout[J]. Arthritis Rheum, 2002,47(4):356-360.
pmid: 12209479 |
| [12] |
Becker MA, Schumacher HR Jr, Wortmann RL, et al. Febuxostat compared with allopurinol in patients with hyperuricemia and gout[J]. N Engl J Med, 2005,353(23):2450-2461.
pmid: 16339094 |
| [13] | Ellmann H, Bayat S, Araujo E, et al. Effects of conventional uric acid lowering therapy on monosodium urate crystal deposits[J]. Arthritis Rheum, 2020,72(1):150-156. |
| [14] |
Wilcox WR, Khalaf AA. Nucleation of monosodium urate crystals[J]. Ann Rheum Dis, 1975,34(4):332-339.
pmid: 242279 |
| [15] |
Simkin PA. The pathogenesis of podagra[J]. Ann Intern Med, 1977,86(2):230-233.
pmid: 319726 |
| [16] | Zhang W, Jin Z, Xiang W, et al. Ultrasonographic features of lower-limb joints in gout: which joints and clinical characteristics would provide more information for diagnosis[J]. J Clin Rheum, 2020,26(1):14-18. |
| [17] |
Dalbeth N, House ME, Aati O, et al. Urate crystal deposition in asymptomatic hyperuricaemia and symptomatic gout: a dual energy CT study[J]. Ann Rheum Dis, 2015,74(5):908-911.
pmid: 25637002 |
| [18] |
Allen DJ, Milosovich G, Mattocks AM. Inhibition of monosodium urate needle crystal growth[J]. Arthritis Rheum, 1965,8(6):1123-1133.
pmid: 5884821 |
| [1] | 甘地, 付强, 唐小惠, 李楚炜, 舒兆平. 胸锁关节痛风1例[J]. 北京大学学报(医学版), 2026, 58(3): 670-673. |
| [2] | 刘伟, 郭稳, 过哲, 李春艳, 李云龙, 刘思奇, 张亮, 宋慧. 痛风患者放射学阴性骨侵蚀的相关危险因素[J]. 北京大学学报(医学版), 2025, 57(4): 735-739. |
| [3] | 方媛媛, 徐帆, 雷杰, 张昊, 张文宇, 孙宇, 吴宏新, 傅开元, 毛伟玉. 基于颞下颌关节紊乱病诊断标准的临床自动诊断系统的建立及验证[J]. 北京大学学报(医学版), 2025, 57(1): 192-201. |
| [4] | 任晓萌,李凯一,李春蕾. 基于转录组测序探索口腔扁平苔藓局部激素治疗敏感性相关分子特征[J]. 北京大学学报(医学版), 2024, 56(1): 32-38. |
| [5] | 董泓,王丽敏,王志强,刘彦卿,张晓刚,张明明,刘娟,李振彬. 急性痛风发作的昼夜差异: 一项男性痛风患者的临床研究[J]. 北京大学学报(医学版), 2023, 55(5): 915-922. |
| [6] | 田雪丽,宋志强,索宝军,周丽雅,李彩玲,张雨欣. 比较Epsilometer试验法和琼脂稀释法检测幽门螺杆菌对甲硝唑的敏感性[J]. 北京大学学报(医学版), 2023, 55(5): 934-938. |
| [7] | 叶一林,刘恒,潘利平,柴卫兵. 全膝关节置换术后假体周围痛风发作误诊1例[J]. 北京大学学报(医学版), 2023, 55(2): 362-365. |
| [8] | 曹瑞洁,姚中强,焦朋清,崔立刚. 不同分类标准对中国大动脉炎的诊断效能比较[J]. 北京大学学报(医学版), 2022, 54(6): 1128-1133. |
| [9] | 王昱,张慧敏,邓雪蓉,刘伟伟,陈璐,赵宁,张晓慧,宋志博,耿研,季兰岚,王玉,张卓莉. 尿枸橼酸定量检测在原发性痛风患者肾结石诊断中的应用价值[J]. 北京大学学报(医学版), 2022, 54(6): 1134-1140. |
| [10] | 谢晓炜,李芬,凌光辉,谢希,许素清,陈谊月. 痛风患者健康教育知识知晓度测量问卷的研制及临床应用[J]. 北京大学学报(医学版), 2022, 54(4): 699-704. |
| [11] | 张学武. 痛风关节炎治疗中几个备受关注的问题[J]. 北京大学学报(医学版), 2021, 53(6): 1017-1019. |
| [12] | 彭喆,丁亚敏,裴林,姚海红,张学武,唐素玫. 痛风患者发生关节及肌腱内晶体沉积的临床特点[J]. 北京大学学报(医学版), 2021, 53(6): 1067-1071. |
| [13] | 王贵红,左婷,李然,左正才. 瑞巴派特在大鼠痛风性关节炎急性发作中的作用[J]. 北京大学学报(医学版), 2021, 53(4): 716-720. |
| [14] | 王昱,邓雪蓉,季兰岚,张晓慧,耿研,张卓莉. 超声检测痛风患者肌腱受累的危险因素和诊断价值[J]. 北京大学学报(医学版), 2021, 53(1): 143-149. |
| [15] | 王鹏,吴华,车颖,范东伟,刘珏,陶立元. 亚洲骨质疏松筛查工具在健康体检中的筛查准确性评价及适宜切点研究[J]. 北京大学学报(医学版), 2019, 51(6): 1085-1090. |
|
||
