北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (4): 647-652. doi: 10.19723/j.issn.1671-167X.2021.04.004
术前血小板参数与局部进展期肾细胞癌预后
肖若陶,刘承,徐楚潇,何为,马潞林( )
)
- 北京大学第三医院泌尿外科,北京 100191
Prognostic value of preoperative platelet parameters in locally advanced renal cell carcinoma
XIAO Ruo-tao,LIU Cheng,XU Chu-xiao,HE Wei,MA Lu-lin()
- Department of Urology, Peking University Third Hospital, Beijing 100191, China
摘要:
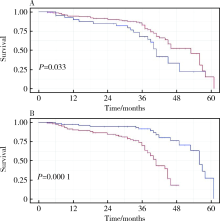
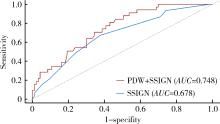
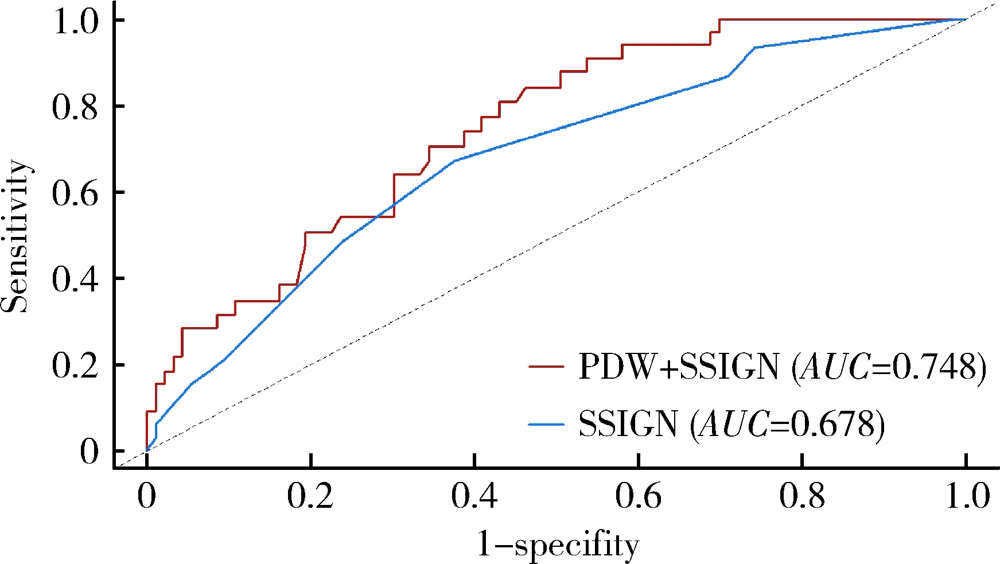
目的: 探讨术前血小板参数对局部进展期肾癌预后的预测价值,为此类患者的危险分层提供参考。方法: 选择北京大学第三医院2015年1月—2017年12月局部进展期肾癌患者进行回顾性分析,依据随访过程中肿瘤是否复发或转移分成进展组和无进展组,比较两组术前血小板参数和临床资料的差异。通过受试者特征工作曲线(receiver operating characteristic curve, ROC)确定血小板参数的最佳临界值,Kaplan-Meier生存曲线分析不同血小板参数与疾病无进展生存时间(progression-free survival, PFS)的关系。通过Cox比例风险模型进行多因素分析确定PFS的独立危险因素。采用时间依赖ROC、净重新分类指数(net reclassification index, NRI)和综合判别改善指数(integrated discrimination improvement, IDI)评估纳入血小板参数后对SSIGN模型改良情况。结果: 共有215例患者入选本研究,其中192例(89.3%)患者获得随访,中位随访时间为36个月。64例(29.8%)患者随访过程中出现疾病进展,中位PFS为46个月。进展组患者的血小板数量(platelet count, PLT)相较无进展组高[(250.72±88.59)×109/L vs. (227.27±66.94)×109/L, P=0.042],血小板分布宽度(platelet distribution width, PDW)相较无进展组低[(12.01±2.27)% vs. (13.31±2.74)%, P=0.001]。将285×109/L及12.65%作为PLT及PDW的最佳临界值,PLT≤285×109/L组患者中位PFS显著长于PLT>285×109/L组(53个月vs. 41个月,P=0.033);PDW>12.65%组患者中位PFS也显著长于PDW≤12.65%组(56个月vs. 41个月,P<0.001)。多因素分析显示术前PDW(HR=0.735, P<0.001)、细胞核分级Ⅲ~Ⅳ级(HR=2.425, P=0.001)、合并肉瘤样分化(HR=3.101, P=0.008)为PFS的独立危险因素。术前PDW联合SSIGN预后评分模型曲线下面积大于原有SSIGN模型[0.748 (95%CI:0.662~0.833) vs. 0.678 (95%CI: 0.583~0.773), P=0.193],NRI为0.262(P=0.04),IDI为 0.085(P=0.01),表明PDW纳入SSIGN模型后其预测能力提高。结论: 术前高PLT和低PDW与局部进展期肾癌不良预后相关,其中PDW是患者预后的独立危险因素,因此,术前PDW有助于对局部进展期肾癌进行危险分层。
中图分类号:
- R737.11

| [1] |
Gay LJ, Felding-Habermann B. Contribution of platelets to tumour metastasis [J]. Nat Rev Cancer, 2011, 11(2):123-134.
doi: 10.1038/nrc3004 |
| [2] |
Labelle M, Begum S, Hynes RO. Direct signaling between platelets and cancer cells induces an epithelial-mesenchymal-like transition and promotes metastasis [J]. Cancer Cell, 2011, 20(5):576-590.
doi: 10.1016/j.ccr.2011.09.009 pmid: 22094253 |
| [3] |
Nieswandt B, Hafner M, Echtenacher B, et al. Lysis of tumor cells by natural killer cells in mice is impeded by platelets [J]. Cancer Res, 1999, 59(6):1295-1300.
pmid: 10096562 |
| [4] |
Zhu X, Cao Y, Lu P, et al. Evaluation of platelet indices as diagnostic biomarkers for colorectal cancer [J]. Sci Rep, 2018, 8(1):11814.
doi: 10.1038/s41598-018-29293-x |
| [5] |
Liu C, Zhang H, Qi Q, et al. The preoperative platelet distribution width: A predictive factor of the prognosis in patients with non-small cell lung cancer [J]. Thorac Cancer, 2020, 11(4):918-927.
doi: 10.1111/tca.v11.4 |
| [6] |
Liu S, Fang J, Jiao D, et al. Elevated platelet count predicts poor prognosis in breast cancer patients with supraclavicular lymph node metastasis [J]. Cancer Manag Res, 2020, 12(6):6069-6075.
doi: 10.2147/CMAR.S257727 |
| [7] |
Heng DY, Xie W, Regan MM, et al. External validation and comparison with other models of the international metastatic renal-cell carcinoma database consortium prognostic model: a population-based study [J]. Lancet Oncol, 2013, 14(2):141-148.
doi: 10.1016/S1470-2045(12)70559-4 |
| [8] |
Choi JY, Ko YH, Song PH. Clinical significance of preoperative thrombocytosis in patients who underwent radical nephrectomy for nonmetastatic renal cell carcinoma [J]. Investig Clin Urol, 2016, 57(5):324-329.
doi: 10.4111/icu.2016.57.5.324 |
| [9] |
Seles M, Posch F, Pichler GP, et al. Blood platelet volume represents a novel prognostic factor in patients with nonmetastatic renal cell carcinoma and improves the predictive ability of established prognostic scores [J]. J Urol, 2017, 198(6):1247-1252.
doi: 10.1016/j.juro.2017.07.036 |
| [10] |
Karakiewicz PI, Trinh QD, Lam JS, et al. Platelet count and preoperative haemoglobin do not significantly increase the performance of established predictors of renal cell carcinoma-specific mortality [J]. Eur Urol, 2007, 52(5):1428-1436.
pmid: 17420085 |
| [11] |
Frank I, Blute ML, Cheville JC, et al. An outcome prediction model for patients with clear cell renal cell carcinoma treated with radical nephrectomy based on tumor stage, size, grade and necrosis: the SSIGN score [J]. J Urol, 2002, 168(6):2395-2400.
doi: 10.1016/S0022-5347(05)64153-5 |
| [12] |
Zisman A, Pantuck AJ, Dorey F, et al. Improved prognostication of renal cell carcinoma using an integrated staging system [J]. J Clin Oncol, 2001, 19(6):1649-1657.
pmid: 11250993 |
| [13] | Amin MB, Edge SB, Greene FL, et al. AJCC cancer staging manual[M]. 8th ed. Chicago: Springer, 2017: 739-747. |
| [14] |
Ljungberg B, Bensalah K, Canfield S, et al. EAU guidelines on renal cell carcinoma: 2014 update [J]. Eur Urol, 2015, 67(5):913-924.
doi: 10.1016/j.eururo.2015.01.005 pmid: 25616710 |
| [15] |
Moch H, Cubilla AL, Humphrey PA, et al. The 2016 WHO classification of tumours of the urinary system and male genital organs-part A: renal, penile, and testicular tumours [J]. Eur Urol, 2016, 70(1):93-105.
doi: 10.1016/j.eururo.2016.02.029 |
| [16] |
Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021 [J]. CA Cancer J Clin, 2021, 71(1):7-33.
doi: 10.3322/caac.v71.1 |
| [17] |
Haas NB, Manola J, Dutcher JP, et al. Adjuvant treatment for high-risk clear cell renal cancer: updated results of a high-risk subset of the ASSURE randomized trial [J]. JAMA Oncol, 2017, 3(9):1249-1252.
doi: 10.1001/jamaoncol.2017.0076 |
| [18] |
Motzer RJ, Haas NB, Donskov F, et al. Randomized phase Ⅲ trial of adjuvant pazopanib versus placebo after nephrectomy in patients with localized or locally advanced renal cell carcinoma [J]. J Clin Oncol, 2017, 35(35):3916-3923.
doi: 10.1200/JCO.2017.73.5324 |
| [19] |
Motzer RJ, Ravaud A, Patard JJ, et al. Adjuvant sunitinib for high-risk renal cell carcinoma after nephrectomy: subgroup analyses and updated overall survival results [J]. Eur Urol, 2018, 73(1):62-68.
doi: 10.1016/j.eururo.2017.09.008 |
| [20] |
Leibovich BC, Blute ML, Cheville JC, et al. Prediction of progression after radical nephrectomy for patients with clear cell renal cell carcinoma: a stratification tool for prospective clinical trials [J]. Cancer, 2003, 97(7):1663-1671.
pmid: 12655523 |
| [21] |
Karakiewicz PI, Briganti A, Chun FK, et al. Multi-institutional validation of a new renal cancer-specific survival nomogram [J]. J Clin Oncol, 2007, 25(11):1316-1322.
pmid: 17416852 |
| [22] |
Correa AF, Jegede O, Haas NB, et al. Predicting renal cancer recurrence: defining limitations of existing prognostic models with prospective trial-based validation [J]. J Clin Oncol, 2019, 37(23):2062-2071.
doi: 10.1200/JCO.19.00107 |
| [23] |
Xiao R, Xu C, He W, et al. Preoperative anaemia and thrombocytosis predict adverse prognosis in non-metastatic renal cell carcinoma with tumour thrombus [J]. BMC Urol, 2021, 21(1):31.
doi: 10.1186/s12894-021-00796-6 |
| [24] |
Yue CX, Liu YX, Yun ZY, et al. Decreased platelet distribution width predicts a worse prognosis in patients undergoing surgical resection for hepatocellular carcinoma [J]. Cancer Biomark, 2019, 26(3):361-366.
doi: 10.3233/CBM-190474 |
| [25] |
Chen H, Wu Q, Zhang Y, et al. Nomograms based on the novel platelet index score predict postoperative prognosis in endometrial cancer [J]. Gynecol Oncol, 2020, 158(3):689-697.
doi: S0090-8258(20)31125-2 pmid: 32507649 |
| [26] |
Kawakita Y, Motoyama S, Sato Y, et al. Prognostic significance of combined platelet distribution width and C-reactive protein score in esophageal cancer [J]. Anticancer Res, 2020, 40(10):5715-5725.
doi: 10.21873/anticanres.14586 pmid: 32988897 |
| [27] | 蒋慧云, 李小毛, 王佳, 等. 术前血小板分布宽度在子宫内膜癌诊断预测中的价值 [J]. 实用医学杂志, 2018, 34(7):1188-1190. |
| [28] |
Vagdatli E, Gounari E, Lazaridou E, et al. Platelet distribution width: a simple, practical and specific marker of activation of coagulation [J]. Hippokratia, 2010, 14(1):28-32.
pmid: 20411056 |
| [29] | 张翔, 庄瑞. 血小板分布宽度对鼻咽癌患者预后的影响 [J]. 国际肿瘤学杂志, 2018, 45(5):257-261. |
| [30] |
Huang Y, Cui MM, Huang YX, et al. Preoperative platelet distribution width predicts breast cancer survival [J]. Cancer Biomark, 2018, 23(2):205-211.
doi: 10.3233/CBM-181267 pmid: 30198864 |
| [31] | 张林楠, 刘玉峰, 苏淑芳, 等. 血小板分布宽度对神经母细胞瘤预后的预测价值 [J]. 中华实用儿科临床杂志, 2020, 35(6):440-444. |
| [1] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [2] | 舒帆, 葛力源, 邓汉彰, 殷昊明, 欧俊永, 邓绍晖, 郝一昌, 陆敏, 张展奕, 段佩辰, 张树栋. 预后不良的肾细胞癌伴淋巴结转移的分子特征[J]. 北京大学学报(医学版), 2026, 58(3): 631-640. |
| [3] | 汤晓菲, 丁秋玲, 张阳, 王育梅, 田美伊, 孙卓, 王荣荣, 陈妍, 刘坚. 阿伐曲泊帕治疗难治性系统性红斑狼疮相关血小板减少1例[J]. 北京大学学报(医学版), 2026, 58(2): 405-409. |
| [4] | 张铃福, 陈明, 赵小宇, 王港, 崔龙, 凌晓锋, 王立新, 徐智, 郭丽梅, 侯纯升. 原发灶局限于胆囊壁内胆囊癌大体分型及其与预后和癌前病变的相关性[J]. 北京大学学报(医学版), 2026, 58(1): 184-189. |
| [5] | 向钊, 杨莉, 杨静. 非靶向代谢组学揭示原发性干燥综合征血小板减少患者血清差异代谢物及代谢通路[J]. 北京大学学报(医学版), 2025, 57(6): 1042-1050. |
| [6] | 高雅静, 李正芳, 马梦思, 武丽君. SII和SIRI对白塞病葡萄膜炎的风险预测及疾病活动度和预后的评估[J]. 北京大学学报(医学版), 2025, 57(6): 1067-1073. |
| [7] | 郭博达, 陆敏, 王国良, 张洪宪, 刘磊, 侯小飞, 赵磊, 田晓军, 张树栋. 肾透明细胞癌与非透明细胞癌伴静脉癌栓患者的临床病理特征及预后比较[J]. 北京大学学报(医学版), 2025, 57(4): 644-649. |
| [8] | 李伟浩, 李晶, 张学民, 李伟, 李清乐, 张小明. 术中回收式自体输血对颈动脉体瘤切除术后肿瘤预后的影响[J]. 北京大学学报(医学版), 2025, 57(2): 272-276. |
| [9] | 毛雅晴, 陈震, 于尧, 章文博, 刘洋, 彭歆. 2型糖尿病对口腔鳞状细胞癌患者预后的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1089-1096. |
| [10] | 张树栋,谢睿扬. 机器人手术时代的肾癌合并腔静脉瘤栓治疗策略[J]. 北京大学学报(医学版), 2024, 56(4): 562-564. |
| [11] | 欧俊永,倪坤明,马潞林,王国良,颜野,杨斌,李庚午,宋昊东,陆敏,叶剑飞,张树栋. 肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素[J]. 北京大学学报(医学版), 2024, 56(4): 582-588. |
| [12] | 刘帅,刘磊,刘茁,张帆,马潞林,田晓军,侯小飞,王国良,赵磊,张树栋. 伴静脉癌栓的肾上腺皮质癌的临床治疗及预后[J]. 北京大学学报(医学版), 2024, 56(4): 624-630. |
| [13] | 虞乐,邓绍晖,张帆,颜野,叶剑飞,张树栋. 具有低度恶性潜能的多房囊性肾肿瘤的临床病理特征及预后[J]. 北京大学学报(医学版), 2024, 56(4): 661-666. |
| [14] | 舒帆,郝一昌,张展奕,邓绍晖,张洪宪,刘磊,王国良,田晓军,赵磊,马潞林,张树栋. 肾部分切除术治疗囊性肾癌的功能学和肿瘤学结果:单中心回顾性研究[J]. 北京大学学报(医学版), 2024, 56(4): 667-672. |
| [15] | 周泽臻,邓绍晖,颜野,张帆,郝一昌,葛力源,张洪宪,王国良,张树栋. 非转移性T3a肾细胞癌患者3年肿瘤特异性生存期预测[J]. 北京大学学报(医学版), 2024, 56(4): 673-679. |
|
||
