北京大学学报(医学版) ›› 2023, Vol. 55 ›› Issue (2): 276-282. doi: 10.19723/j.issn.1671-167X.2023.02.011
肾黏液样小管状和梭形细胞癌的临床病理特点及预后
沈棋*( ),刘亿骁,何群
),刘亿骁,何群
- 北京大学第一医院泌尿外科, 北京大学泌尿外科研究所, 国家泌尿、男性生殖系肿瘤研究中心, 北京 100034
Mucinous tubular and spindle cell carcinoma of kidney: Clinicopathology and prognosis
Qi SHEN*(),Yi-xiao LIU,Qun HE
- Department of Urology, Peking University First Hospital; Institute of Urology, Peking University; National Urological Cancer Center, Beijing 100034, China
摘要:
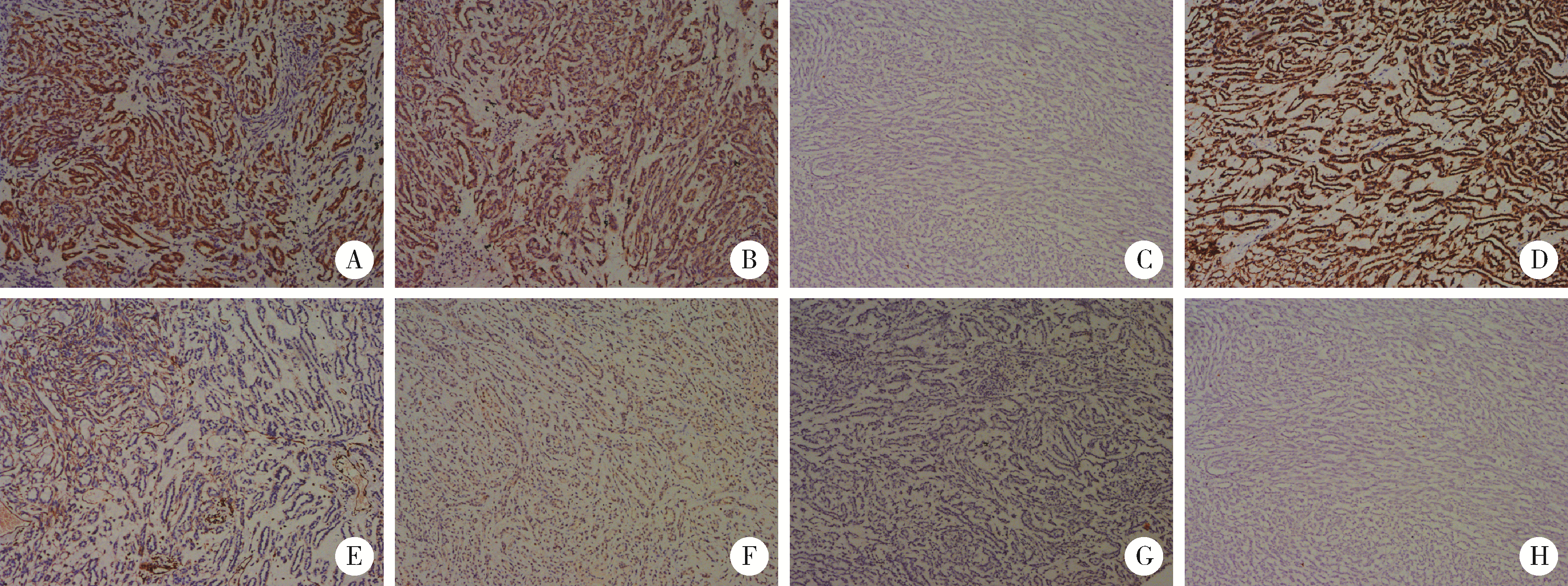
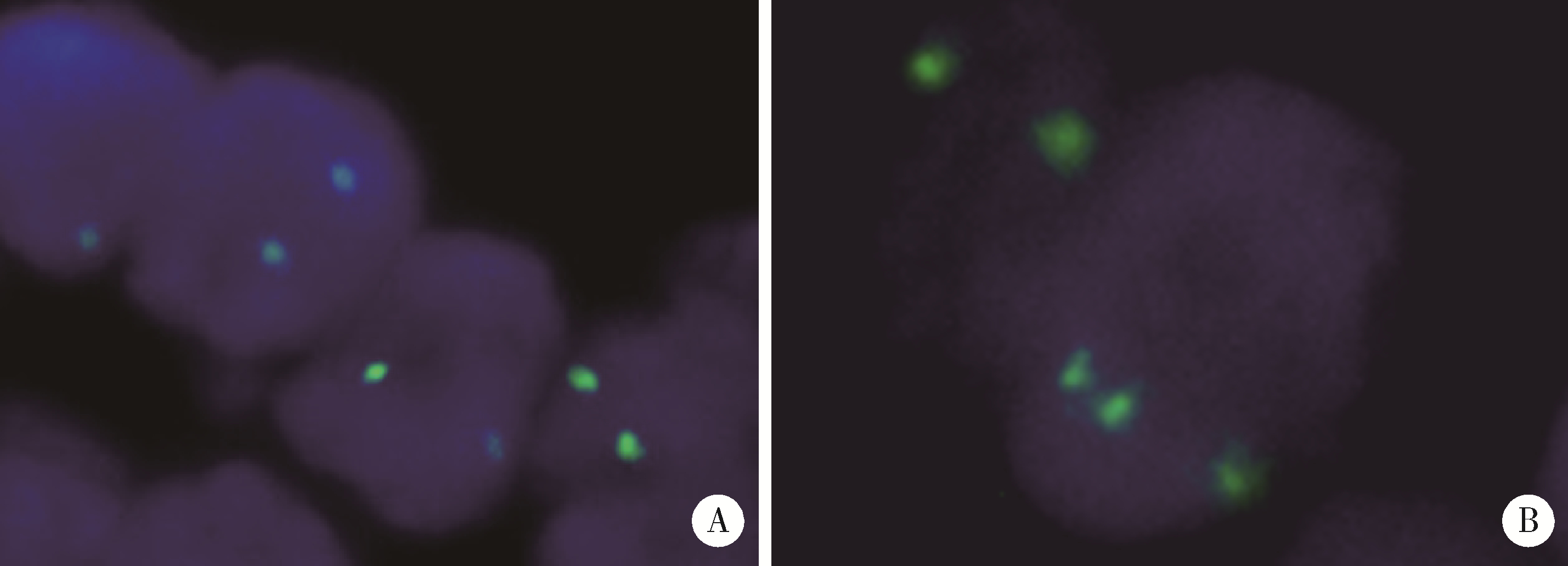
目的: 探讨肾黏液样小管状和梭形细胞癌的临床病理学特征、免疫表型、鉴别诊断及预后。方法: 回顾性分析13例肾黏液样小管状和梭形细胞癌病例, 总结其临床和病理学特点以及免疫组织化学表达情况, 并进行荧光原位杂交检测。结果: 13例患者年龄39~78岁, 平均57.1岁, 其中男性4例, 女性9例, 男女比例为1 ∶2.25, 均无临床症状, 为偶然发现。3例行肾部分切除术, 10例行肾根治切除术; 9例肿瘤位于左侧肾, 4例位于右侧肾, 最大径2~12 cm。大部分病例镜下形态为经典型形态改变, 细胞核分级采用世界卫生组织(World Health Organization, WHO)/国际泌尿病理协会(International Society of Urological Pathology, ISUP)分级系统, 11例为G2, 2例为G3。病理分期PT1a共6例, PT1b共3例, PT2a共2例, PT2b及PT3a各1例。免疫组织化学染色阳性率: 波形蛋白(vimentin)、AE1/AE3、α-甲基脂酰辅酶A消旋酶(α-methylacyl-CoA racemase, αMACR)、细胞角蛋白(cytokeratin, CK)8/18均为100%(13/13), CK7为92.3%(12/13), 上皮细胞膜抗原(epithelial membrane antigen, EMA)为92.3%(12/13), CK20为46.2%(6/13), CD10为30.8%(4/13), 突触素(synaptophysin, Syn)为7.7%(1/13), 嗜铬素(chromogranin A, CgA)、CD57、WT1、Ki-67均为0(0/13)。荧光原位杂交结果显示所有病例均未见7、17号染色体多倍体改变。术后随访6个月至7年6个月, 2例出现肺转移后死亡(1例核分级为G3, 1例伴有坏死), 其余11例无复发和转移。结论: 肾黏液样小管状和梭形细胞癌是一种低度恶性的独特类型肾肿瘤, 好发于女性, 年龄分布广泛。目前治疗方法为手术切除, 伴有坏死及高级别形态的病例易发生复发和转移, 虽然大部分病例预后良好, 但术后仍需密切随访。
中图分类号:
- R737.11



| 1 | Eble JN, Sauter G, Epstein JI, et al. World Health Organization classification of tumours: Pathology and genetics of tumours of the urinary system and male genital organs[R]. Lyon, France: International Agency for Research on Cancer, 2004. |
| 2 | Moch H, Humphrey P, Ulbright T, et al. World Health Organization classification of tumours of the urinary system and male genital organs[R]. Lyon, France: International Agency for Research on Cancer, 2016. |
| 3 |
MacLennan GT , Farrow GM , Bostwick DG . Low-grade collecting duct carcinoma of the kidney: Report of 13 cases of low-grade mucinous tubulocystic renal carcinoma of possible collecting duct origin[J]. Urology, 1997, 50 (5): 679- 684.
doi: 10.1016/S0090-4295(97)00335-X |
| 4 |
Ged Y , Chen YB , Knezevic A , et al. Mucinous tubular and spindle-cell carcinoma of the kidney: Clinical features, genomic profiles, and treatment outcomes[J]. Clin Genitourin Cancer, 2019, 17 (4): 268- 274.
doi: 10.1016/j.clgc.2019.04.006 |
| 5 |
Xu X , Zhong J , Zhou X , et al. Mucinous tubular and spindle cell carcinoma of the kidney: A study of clinical, imaging features and treatment outcomes[J]. Front Oncol, 2022, 12, 865263.
doi: 10.3389/fonc.2022.865263 |
| 6 |
Ferlicot S , Allory Y , Comperat E , et al. Mucinous tubular and spindle cell carcinoma: A report of 15 cases and a review of the literature[J]. Virchows Arch, 2005, 447 (6): 978- 983.
doi: 10.1007/s00428-005-0036-x |
| 7 |
Rakozy C , Schmahl GE , Bogner S , et al. Low-grade tubular-mucinous renal neoplasms: Morphologic, immunohistochemical, and genetic features[J]. Mod Pathol, 2002, 15 (11): 1162- 1171.
doi: 10.1097/01.MP.0000031709.40712.46 |
| 8 |
Nathany S , Monappa V . Mucinous tubular and spindle cell carcinoma: A review of histopathology and clinical and prognostic implications[J]. Arch Pathol Lab Med, 2020, 144 (1): 115- 118.
doi: 10.5858/arpa.2017-0506-RS |
| 9 | Xiao L , Xiao W , Guo Y , et al. Huge mucinous tubular and spindle cell carcinoma of the kidney: A case report[J]. Urol Case Rep, 2021, 40, 101914. |
| 10 |
Bajpai M , Pooja S , Tyagi M , et al. Mucinous spindle and tubular renal cell cancer: A rare variant of renal cell cancer[J]. J Cancer Res Ther, 2022, 18 (4): 1168- 1170.
doi: 10.4103/jcrt.jcrt_99_21 |
| 11 | Kuroda N , Hes O , Michal M , et al. Mucinous tubular and spindle cell carcinoma with Fuhrman nuclear grade 3: A histological, immunohistochemical, ultrastructural and FISH study[J]. Histol Histopathol, 2008, 23 (12): 1517- 1523. |
| 12 |
Fuchizawa H , Kijima T , Takada-Owada A , et al. Metastatic mucinous tubular and spindle cell carcinoma of the kidney responding to nivolumab plus ipilimumab[J]. IJU Case Rep, 2021, 4 (5): 333- 337.
doi: 10.1002/iju5.12342 |
| 13 |
Arafah M , Zaidi SN . Mucinous tubular and spindle cell carcinoma of the kidney with sarcomatoid transformation[J]. Saudi J Kidney Dis Transplant, 2013, 24 (3): 557- 560.
doi: 10.4103/1319-2442.111066 |
| 14 |
Bulimbasic S , Ljubanovic D , Sima R , et al. Aggressive high-grade mucinous tubular and spindle cell carcinoma[J]. Hum Pathol, 2009, 40 (6): 906- 907.
doi: 10.1016/j.humpath.2009.03.004 |
| 15 |
Pillay N , Ramdial PK , Cooper K , et al. Mucinous tubular and spindle cell carcinoma with aggressive histomorphology: A sarco-matoid variant[J]. Hum Pathol, 2008, 39 (6): 966- 969.
doi: 10.1016/j.humpath.2007.10.006 |
| 16 | Simon RA , di Sant'agnese PA , Palapattu GS , et al. Mucinous tubular and spindle cell carcinoma of the kidney with sarcomatoid differentiation[J]. Int J Clin Exp Pathol, 2008, 1 (2): 180- 184. |
| 17 |
Dhillon J , Amin MB , Selbs E , et al. Mucinous tubular and spindle cell carcinoma of the kidney with sarcomatoid change[J]. Am J Surg Pathol, 2009, 33 (1): 44- 49.
doi: 10.1097/PAS.0b013e3181829ed5 |
| 18 |
Fine SW , Argani P , DeMarzo AM , et al. Expanding the histologic spectrum of mucinous tubular and spindle cell carcinoma of the kidney[J]. Am J Surg Pathol, 2006, 30, 1554- 1560.
doi: 10.1097/01.pas.0000213271.15221.e3 |
| 19 |
Reuter VE , Argani P , Zhou M , et al. Best practices recommendations in the application of immunohistochemistry in the kidney tumors: Report from the International Society of Urologic Pathology[J]. Am J Surg Pathol, 2014, 38 (8): e35- e49.
doi: 10.1097/PAS.0000000000000258 |
| 20 |
Paner GP , Srigley JR , Radhakrishnan A , et al. Immunohistochemical analysis of mucinous tubular and spindle cell carcinoma and papillary renal cell carcinoma of the kidney: Significant immunophenotypic overlap warrants diagnostic caution[J]. Am J Surg Pathol, 2006, 30 (1): 13- 19.
doi: 10.1097/01.pas.0000180443.94645.50 |
| 21 |
Uchida S , Suzuki K , Uno M , et al. Mucin-poor and aggressive mucinous tubular and spindle cell carcinoma of the kidney: Two case reports[J]. Mol Clin Oncol, 2017, 7 (5): 777- 782.
doi: 10.3892/mco.2017.1400 |
| 22 |
Kuroda N , Nakamura S , Miyazaki E , et al. Low-grade tubular-mucinous renal neoplasm with neuroendocrine differentiation: A histological, immunohistochemical and ultrastructural study[J]. Pathol Int, 2004, 54 (3): 201- 207.
doi: 10.1111/j.1440-1827.2004.01608.x |
| 23 |
Peckova K , Martinek P , Sperga M , et al. Mucinous spindle and tubular renal cell carcinoma: Analysis of chromosomal aberration pattern of low-grade, high grade, and an overlapping morphologic variant with papillary renal[J]. Ann Diagn Pathol, 2015, 19 (4): 226- 231.
doi: 10.1016/j.anndiagpath.2015.04.004 |
| 24 |
Kuroda N , Naroda T , Tamura M , et al. High-grade mucinous tubular and spindle cell carcinoma: Comparative genomic hybridization study[J]. Ann Diagn Pathol, 2011, 15 (6): 472- 475.
doi: 10.1016/j.anndiagpath.2010.08.003 |
| 25 |
Sadimin ET , Chen YB , Wang L , et al. Chromosomal abnormalities of high-grade mucinous tubular and spindle cell carcinoma of the kidney[J]. Histopathology, 2017, 71 (5): 719- 724.
doi: 10.1111/his.13298 |
| 26 |
Mehra R , Vats P , Cieslik M , et al. Bi-allelic alteration and dysregulation of the Hippo pathway in mucinous tubular and spindle cell carcinoma of the kidney[J]. Cancer Discov, 2016, 6 (11): 1258- 1266.
doi: 10.1158/2159-8290.CD-16-0267 |
| 27 |
Ren Q , Wang L , Al-Ahmadie HA , et al. Distinct genomic copy number alterations distinguish mucinous tubular and spindle cell carcinoma of the kidney from papillary renal cell carcinoma with overlapping histologic features[J]. Am J Surg Pathol, 2018, 42 (6): 767- 777.
doi: 10.1097/PAS.0000000000001038 |
| 28 |
邹子归, 王玉红, 周晋星, 等. 肾黏液样小管状和梭形细胞癌临床病理分析及全外显子组测序分析[J]. 中华病理学杂志, 2021, 50 (7): 762- 767.
doi: 10.3760/cma.j.cn112151-20200922-00731 |
| 29 |
Xu H , Li W , Zhu C , et al. Proteomic profiling identifies novel diagnostic biomarkers and molecular subtypes for mucinous tubular and spindle cell carcinoma of the kidney[J]. J Pathol, 2022, 257 (1): 53- 67.
doi: 10.1002/path.5869 |
| 30 |
Bharti JN , Choudhary GR , Madduri VKS , et al. Mucinous tubular and spindle cell carcinoma: A difficult diagnosis[J]. Urol Ann, 2021, 13 (2): 180- 182.
doi: 10.4103/UA.UA_44_20 |
| 31 |
Thway K , du Parcq J , Larkin JM , et al. Metastatic renal muci-nous tubular and spindle cell carcinoma. Atypical behavior of a rare, morphologically bland tumor[J]. Ann Diagn Pathol, 2012, 16 (5): 407- 410.
doi: 10.1016/j.anndiagpath.2011.04.001 |
| 32 |
Cossu-Rocca P , Eble JN , Delahunt B , et al. Renal mucinous tubular and spindle carcinoma lacks the gains of chromosomes 7 and 17 and losses of chromosome Y that are prevalent in papillary renal cell carcinoma[J]. Mod Pathol, 2006, 19 (4): 488- 493.
doi: 10.1038/modpathol.3800565 |
| [1] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [2] | 舒帆, 葛力源, 邓汉彰, 殷昊明, 欧俊永, 邓绍晖, 郝一昌, 陆敏, 张展奕, 段佩辰, 张树栋. 预后不良的肾细胞癌伴淋巴结转移的分子特征[J]. 北京大学学报(医学版), 2026, 58(3): 631-640. |
| [3] | 张铃福, 陈明, 赵小宇, 王港, 崔龙, 凌晓锋, 王立新, 徐智, 郭丽梅, 侯纯升. 原发灶局限于胆囊壁内胆囊癌大体分型及其与预后和癌前病变的相关性[J]. 北京大学学报(医学版), 2026, 58(1): 184-189. |
| [4] | 赵业, 刁小莉, 熊焰. 细胞转移技术在微量细胞液病理诊断中的应用[J]. 北京大学学报(医学版), 2026, 58(1): 208-213. |
| [5] | 高雅静, 李正芳, 马梦思, 武丽君. SII和SIRI对白塞病葡萄膜炎的风险预测及疾病活动度和预后的评估[J]. 北京大学学报(医学版), 2025, 57(6): 1067-1073. |
| [6] | 王晓林, 李璐瑶, 张雯, 王鸿雁. 3例子宫体中肾样腺癌的临床病理学分析[J]. 北京大学学报(医学版), 2025, 57(6): 1208-1212. |
| [7] | 郭博达, 陆敏, 王国良, 张洪宪, 刘磊, 侯小飞, 赵磊, 田晓军, 张树栋. 肾透明细胞癌与非透明细胞癌伴静脉癌栓患者的临床病理特征及预后比较[J]. 北京大学学报(医学版), 2025, 57(4): 644-649. |
| [8] | 张展奕, 陆敏, 孙悦皓, 董靖晗, 侯小飞, 肖春雷, 王国良, 田晓军, 马潞林, 张洪宪, 张树栋. TFE3重排肾细胞癌合并静脉癌栓患者的临床病理特征及生存分析[J]. 北京大学学报(医学版), 2025, 57(4): 650-661. |
| [9] | 周泽臻, 葛力源, 张帆, 邓绍晖, 颜野, 张洪宪, 王国良, 刘磊, 黄毅, 张树栋. 病理T3a期肾细胞癌肾部分切除与根治性肾切除的回顾性匹配研究[J]. 北京大学学报(医学版), 2025, 57(4): 704-710. |
| [10] | 李伟浩, 李晶, 张学民, 李伟, 李清乐, 张小明. 术中回收式自体输血对颈动脉体瘤切除术后肿瘤预后的影响[J]. 北京大学学报(医学版), 2025, 57(2): 272-276. |
| [11] | 毛雅晴, 陈震, 于尧, 章文博, 刘洋, 彭歆. 2型糖尿病对口腔鳞状细胞癌患者预后的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1089-1096. |
| [12] | 欧俊永,倪坤明,马潞林,王国良,颜野,杨斌,李庚午,宋昊东,陆敏,叶剑飞,张树栋. 肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素[J]. 北京大学学报(医学版), 2024, 56(4): 582-588. |
| [13] | 刘帅,刘磊,刘茁,张帆,马潞林,田晓军,侯小飞,王国良,赵磊,张树栋. 伴静脉癌栓的肾上腺皮质癌的临床治疗及预后[J]. 北京大学学报(医学版), 2024, 56(4): 624-630. |
| [14] | 虞乐,邓绍晖,张帆,颜野,叶剑飞,张树栋. 具有低度恶性潜能的多房囊性肾肿瘤的临床病理特征及预后[J]. 北京大学学报(医学版), 2024, 56(4): 661-666. |
| [15] | 周泽臻,邓绍晖,颜野,张帆,郝一昌,葛力源,张洪宪,王国良,张树栋. 非转移性T3a肾细胞癌患者3年肿瘤特异性生存期预测[J]. 北京大学学报(医学版), 2024, 56(4): 673-679. |
|
||
