北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (4): 640-646. doi: 10.19723/j.issn.1671-167X.2021.04.003
延胡索酸水合酶缺陷型肾细胞癌的临床病理特征及预后
于妍斐,何世明,吴宇财,熊盛炜,沈棋,李妍妍,杨风,何群( ),李学松()
),李学松()
- 北京大学第一医院泌尿外科,北京大学泌尿外科研究所,国家泌尿、男性生殖系肿瘤研究中心,北京 100034
Clinicopathological features and prognosis of fumarate hydratase deficient renal cell carcinoma
YU Yan-fei,HE Shi-ming,WU Yu-cai,XIONG Sheng-wei,SHEN Qi,LI Yan-yan,YANG Feng,HE Qun(),LI Xue-song()
- National Urological Cancer Center, Beijing 100034, China
摘要:
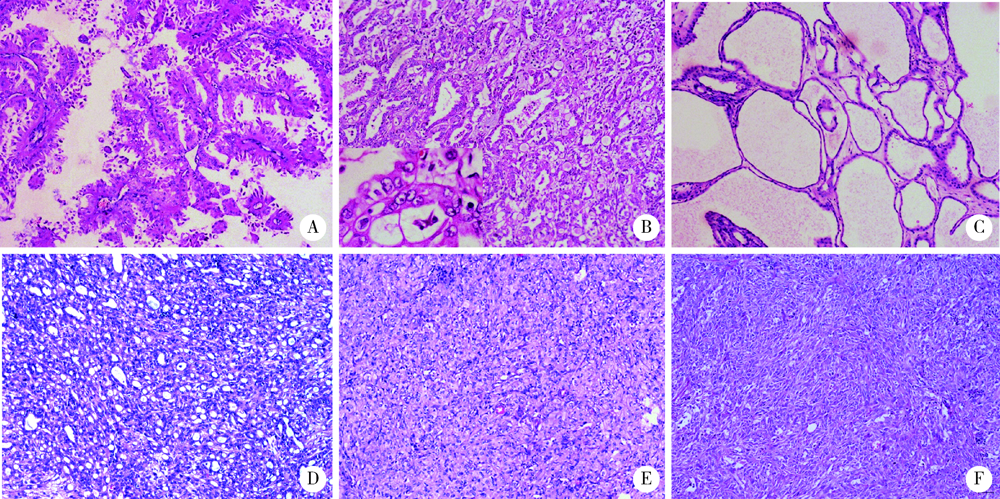
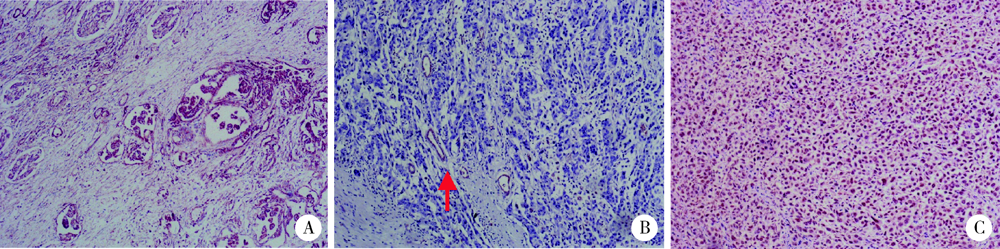
目的: 探讨延胡索酸水合酶缺陷型肾细胞癌(fumarate hydratase-deficient renal cell carcinoma,FH-RCC)的临床病理特征及预后。方法: 应用免疫组织化学染色的方法检测北京大学第一医院泌尿外科2013年1月至2019年12月收治的109例60岁及以下不同类型肾细胞癌患者肿瘤组织中延胡索酸水合酶(fumarate hydratase,FH)的表达情况,分析FH-RCC的临床病理特征及预后。结果: 筛选出11例FH-RCC患者,其中男性7例,女性4例,发病年龄16~53岁(平均36.7岁)。4名女性患者均有子宫肌瘤病史,仅1例患者的一级亲属有肾癌家族史,所有患者均无皮肤平滑肌肿瘤的病史及家族史。肾细胞癌的肿瘤直径2.1~12.0 cm(平均8.83 cm), 9例患者有肾窦或肾周脂肪侵犯,6例有肾静脉或下腔静脉内瘤栓形成,7例有淋巴结转移,4例侵犯肾上腺,1例侵犯脾脏被膜。11例患者中7例(7/49例,14.3%)原诊断为Ⅱ型乳头状肾细胞癌,2例(2/9例,22.2%)原诊断为集合管癌,2例(2/51例,3.9%)原诊断为未分类型肾细胞癌。肿瘤组织病理学大多表现为乳头状、管囊状、实性片状等不同结构的混合,最常见的组织结构为乳头状(9/11例,81.8%)及管状(8/11例,72.7%)结构,3例伴有肉瘤样分化。肿瘤细胞均可见灶状分布大而明显的嗜酸性核仁(WHO/国际泌尿病理协会Ⅲ~Ⅳ级)及核周空晕。免疫组织化学检测显示,癌组织CA9、CD10、CK7染色大多阴性,2例TFE3阳性表达的病例经荧光原位杂交技术(fluorescence in situ hybridization,FISH)检测,结果显示TFE3基因均未发生易位或扩增。11例患者均获得随访资料,随访时间11~82个月,确诊后患者平均生存期为24个月,其中5例于术后9~31个月(平均19个月)因肿瘤远处转移而死亡,6例存活患者中已有5例发生了远处转移。结论: FH-RCC在组织形态学上与多种肾细胞癌有重叠,乳头状及管囊状排列方式的混合存在是FH-RCC最常见的生长方式,癌细胞中灶状出现大而明显的嗜酸性核仁是该类型肾细胞癌的重要组织学特征,FH免疫组织化学染色有助于明确诊断。对于患有平滑肌瘤的年轻女性肾细胞癌患者,需警惕FH-RCC的可能。部分FH-RCC的诊断缺少临床证据,应根据组织病理学特征进一步行基因检测以确诊。
中图分类号:
- R737.11


| [1] |
Pivovarcikova K, Martinek P, Grossmann P, et al. Fumarate hydratase deficient renal cell carcinoma: Chromosomal numerical aberration analysis of 12 cases [J]. Ann Diagn Pathol, 2019, 39:63-68.
doi: S1092-9134(19)30031-0 pmid: 30785029 |
| [2] | 周婷婷, 邢金春. FH基因在遗传性平滑肌瘤病及肾癌综合征中的研究进展 [J]. 医学综述, 2014, 20(5):881-884. |
| [3] |
Alam NA, Bevan S, Churchman M, et al. Localization of a gene (MCUL1) for multiple cutaneous leiomyomata and uterine fibroids to chromosome 1q42.3-q43 [J]. Am J Hum Genet, 2001, 68(5):1264-1269.
pmid: 11283798 |
| [4] |
Tomlinson IP, Alam NA, Rowan AJ, et al. Germline mutations in FH predispose to dominantly inherited uterine fibroids, skin leiomyomata and papillary renal cell cancer [J]. Nat Genet, 2002, 30(4):406-410.
pmid: 11865300 |
| [5] | Hansen AW, Chayed Z, Pallesen K, et al. Hereditary leiomyomatosis and renal cell cancer [J]. Acta Derm Venereol, 2020, 100(1): adv00012. |
| [6] |
Chen YB, Brannon AR, Toubaji A, et al. Hereditary leiomyomatosis and renal cell carcinoma syndrome-associated renal cancer: Recognition of the syndrome by pathologic features and the utility of detecting aberrant succination by immunohistochemistry [J]. Am J Surg Pathol, 2014, 38(5):627-637.
doi: 10.1097/PAS.0000000000000163 |
| [7] |
Patel VM, Handler MZ, Schwartz RA, et al. Hereditary leiomyomatosis and renal cell cancer syndrome: An update and review [J]. J Am Acad Dermatol, 2017, 77(1):149-158.
doi: 10.1016/j.jaad.2017.01.023 |
| [8] | Alam NA, Barclay E, Rowan AJ, et al. Clinical features of multiple cutaneous and uterine leiomyomatosis: An underdiagnosed tumor syndrome [J]. Arch Dermatol, 2005, 141(2):199-206. |
| [9] |
Wei MH, Toure O, Glenn GM, et al. Novel mutations in FH and expansion of the spectrum of phenotypes expressed in families with hereditary leiomyomatosis and renal cell cancer [J]. J Med Genet, 2006, 43(1):18-27.
pmid: 15937070 |
| [10] |
Menko FH, Maher ER, Schmidt LS, et al. Hereditary leiomyomatosis and renal cell cancer (HLRCC): Renal cancer risk, surveillance and treatment [J]. Fam Cancer, 2014, 13(4):637-644.
doi: 10.1007/s10689-014-9735-2 pmid: 25012257 |
| [11] |
Ooi A. Advances in hereditary leiomyomatosis and renal cell carcinoma (HLRCC) research [J]. Semin Cancer Biol, 2020, 61:158-166.
doi: 10.1016/j.semcancer.2019.10.016 |
| [12] |
Alam NA, Rowan AJ, Wortham NC, et al. Genetic and functional analyses of FH mutations in multiple cutaneous and uterine leiomyomatosis, hereditary leiomyomatosis and renal cancer, and fumarate hydratase deficiency [J]. Hum Mol Genet, 2003, 12(11):1241-1252.
pmid: 12761039 |
| [13] |
Lehtonen HJ. Hereditary leiomyomatosis and renal cell cancer: update on clinical and molecular characteristics [J]. Fam Cancer, 2011, 10(2):397-411.
doi: 10.1007/s10689-011-9428-z pmid: 21404119 |
| [14] |
Lau HD, Chan E, Fan AC, et al. A clinicopathologic and mole-cular analysis of fumarate hydratase-deficient renal cell carcinoma in 32 patients [J]. Am J Surg Pathol, 2020, 44(1):98-110.
doi: 10.1097/PAS.0000000000001372 |
| [15] |
Muller M, Ferlicot S, Guillaud-Bataille M, et al. Reassessing the clinical spectrum associated with hereditary leiomyomatosis and renal cell carcinoma syndrome in French FH mutation carriers [J]. Clin Genet, 2017, 92(6):606-615.
doi: 10.1111/cge.13014 pmid: 28300276 |
| [16] |
Alderson NL, Wang Y, Blatnik M, et al. S-(2-succinyl)cys-teine: A novel chemical modification of tissue proteins by a Krebs cycle intermediate [J]. Arch Biochem Biophys, 2006, 450(1):1-8.
pmid: 16624247 |
| [17] |
Gupta S, Swanson AA, Chen Y, et al. Incidence of succinate dehydrogenase and fumarate hydratase-deficient renal cell carcinoma based on immunohistochemical screening with SDHA/SDHB and FH/2SC [J]. Hum Pathol, 2019, 91:114-122.
doi: 10.1016/j.humpath.2019.07.004 |
| [18] |
Trpkov K, Hes O, Agaimy A, et al. Fumarate hydratase-deficient renal cell carcinoma is strongly correlated with fumarate hydratase mutation and hereditary leiomyomatosis and renal cell carcinoma syndrome [J]. Am J Surg Pathol, 2016, 40(7):865-875.
doi: 10.1097/PAS.0000000000000617 pmid: 26900816 |
| [19] |
Muller M, Guillaud-Bataille M, Salleron J, et al. Pattern multiplicity and fumarate hydratase (FH)/S-(2-succino)-cysteine (2SC) staining but not eosinophilic nucleoli with perinucleolar halos differentiate hereditary leiomyomatosis and renal cell carcinoma-associated renal cell carcinomas from kidney tumors without FH gene alteration [J]. Mod Pathol, 2018, 31(6):974-983.
doi: 10.1038/s41379-018-0017-7 |
| [20] |
Wong MH, Tan CS, Lee SC, et al. Potential genetic anticipation in hereditary leiomyomatosis-renal cell cancer (HLRCC) [J]. Fam Cancer, 2014, 13(2):281-289.
doi: 10.1007/s10689-014-9703-x pmid: 24526232 |
| [21] |
Toro JR, Nickerson ML, Wei MH, et al. Mutations in the fuma-rate hydratase gene cause hereditary leiomyomatosis and renal cell cancer in families in North America [J]. Am J Hum Genet, 2003, 73(1):95-106.
doi: 10.1086/376435 |
| [22] |
Hol JA, Jongmans MCJ, Littooij AS, et al. Renal cell carcinoma in young FH mutation carriers: case series and review of the literature [J]. Fam Cancer, 2020, 19(1):55-63.
doi: 10.1007/s10689-019-00155-3 pmid: 31792767 |
| [23] |
Merino MJ, Torres-Cabala C, Pinto P, et al. The morphologic spectrum of kidney tumors in hereditary leiomyomatosis and renal cell carcinoma (HLRCC) syndrome [J]. Am J Surg Pathol, 2007, 31(10):1578-1585.
pmid: 17895761 |
| [24] |
Moch H, Cubilla AL, Humphrey PA, et al. The 2016 WHO classification of tumours of the urinary system and male genital organs: part A: renal, penile, and testicular tumours [J]. Eur Urol, 2016, 70(1):93-105.
doi: 10.1016/j.eururo.2016.02.029 |
| [25] |
Ohe C, Smith SC, Sirohi D, et al. Reappraisal of morphologic differences between renal medullary carcinoma, collecting duct carcinoma, and fumarate hydratase-deficient renal cell carcinoma [J]. Am J Surg Pathol, 2018, 42(3):279-292.
doi: 10.1097/PAS.0000000000001000 |
| [26] |
Smith SC, Trpkov K, Chen YB, et al. Tubulocystic carcinoma of the kidney with poorly differentiated foci: A frequent morphologic pattern of fumarate hydratase-deficient renal cell carcinoma [J]. Am J Surg Pathol, 2016, 40(11):1457-1472.
doi: 10.1097/PAS.0000000000000719 |
| [27] | Forde C, Lim D, Alwan Y, et al. Hereditary leiomyomatosis and renal cell cancer: Clinical, molecular, and screening features in a cohort of 185 affected individuals [J]. Eur Urol Oncol, 2020, 3(6):764-772. |
| [28] |
Smith SC, Sirohi D, Ohe C, et al. A distinctive, low-grade oncocytic fumarate hydratase-deficient renal cell carcinoma, morpholo-gically reminiscent of succinate dehydrogenase-deficient renal cell carcinoma [J]. Histopathology, 2017, 71(1):42-52.
doi: 10.1111/his.2017.71.issue-1 |
| [29] |
Launonen V, Vierimaa O, Kiuru M, et al. Inherited susceptibility to uterine leiomyomas and renal cell cancer [J]. Proc Natl Acad Sci USA, 2001, 98(6):3387-3392.
doi: 10.1073/pnas.051633798 |
| [30] |
Choi Y, Keam B, Kim M, et al. Bevacizumab plus erlotinib combination therapy for advanced hereditary leiomyomatosis and renal cell carcinoma-associated renal cell carcinoma: A multicenter retrospective analysis in Korean patients [J]. Cancer Res Treat, 2019, 51(4):1549-1556.
doi: 10.4143/crt.2019.086 |
| [31] |
Verine J, Pluvinage A, Bousquet G, et al. Hereditary renal cancer syndromes: An update of a systematic review [J]. Eur Urol, 2010, 58(5):701-710.
doi: 10.1016/j.eururo.2010.08.031 |
| [32] |
Joly D, Mejean A, Correas JM, et al. Progress in nephron sparing therapy for renal cell carcinoma and von Hippel-Lindau disease [J]. J Urol, 2011, 185(6):2056-2060.
doi: 10.1016/j.juro.2011.02.007 |
| [33] |
Benson AB, Venook AP, Al-Hawary MM, et al. Rectal cancer, version 2. 2018, NCCN clinical practice guidelines in oncology [J]. J Natl Compr Canc Netw, 2018, 16(7):874-901.
doi: 10.6004/jnccn.2018.0061 |
| [1] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [2] | 舒帆, 葛力源, 邓汉彰, 殷昊明, 欧俊永, 邓绍晖, 郝一昌, 陆敏, 张展奕, 段佩辰, 张树栋. 预后不良的肾细胞癌伴淋巴结转移的分子特征[J]. 北京大学学报(医学版), 2026, 58(3): 631-640. |
| [3] | 张铃福, 陈明, 赵小宇, 王港, 崔龙, 凌晓锋, 王立新, 徐智, 郭丽梅, 侯纯升. 原发灶局限于胆囊壁内胆囊癌大体分型及其与预后和癌前病变的相关性[J]. 北京大学学报(医学版), 2026, 58(1): 184-189. |
| [4] | 赵业, 刁小莉, 熊焰. 细胞转移技术在微量细胞液病理诊断中的应用[J]. 北京大学学报(医学版), 2026, 58(1): 208-213. |
| [5] | 高雅静, 李正芳, 马梦思, 武丽君. SII和SIRI对白塞病葡萄膜炎的风险预测及疾病活动度和预后的评估[J]. 北京大学学报(医学版), 2025, 57(6): 1067-1073. |
| [6] | 郭博达, 陆敏, 王国良, 张洪宪, 刘磊, 侯小飞, 赵磊, 田晓军, 张树栋. 肾透明细胞癌与非透明细胞癌伴静脉癌栓患者的临床病理特征及预后比较[J]. 北京大学学报(医学版), 2025, 57(4): 644-649. |
| [7] | 张展奕, 陆敏, 孙悦皓, 董靖晗, 侯小飞, 肖春雷, 王国良, 田晓军, 马潞林, 张洪宪, 张树栋. TFE3重排肾细胞癌合并静脉癌栓患者的临床病理特征及生存分析[J]. 北京大学学报(医学版), 2025, 57(4): 650-661. |
| [8] | 周泽臻, 葛力源, 张帆, 邓绍晖, 颜野, 张洪宪, 王国良, 刘磊, 黄毅, 张树栋. 病理T3a期肾细胞癌肾部分切除与根治性肾切除的回顾性匹配研究[J]. 北京大学学报(医学版), 2025, 57(4): 704-710. |
| [9] | 李伟浩, 李晶, 张学民, 李伟, 李清乐, 张小明. 术中回收式自体输血对颈动脉体瘤切除术后肿瘤预后的影响[J]. 北京大学学报(医学版), 2025, 57(2): 272-276. |
| [10] | 毛雅晴, 陈震, 于尧, 章文博, 刘洋, 彭歆. 2型糖尿病对口腔鳞状细胞癌患者预后的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1089-1096. |
| [11] | 欧俊永,倪坤明,马潞林,王国良,颜野,杨斌,李庚午,宋昊东,陆敏,叶剑飞,张树栋. 肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素[J]. 北京大学学报(医学版), 2024, 56(4): 582-588. |
| [12] | 刘帅,刘磊,刘茁,张帆,马潞林,田晓军,侯小飞,王国良,赵磊,张树栋. 伴静脉癌栓的肾上腺皮质癌的临床治疗及预后[J]. 北京大学学报(医学版), 2024, 56(4): 624-630. |
| [13] | 虞乐,邓绍晖,张帆,颜野,叶剑飞,张树栋. 具有低度恶性潜能的多房囊性肾肿瘤的临床病理特征及预后[J]. 北京大学学报(医学版), 2024, 56(4): 661-666. |
| [14] | 周泽臻,邓绍晖,颜野,张帆,郝一昌,葛力源,张洪宪,王国良,张树栋. 非转移性T3a肾细胞癌患者3年肿瘤特异性生存期预测[J]. 北京大学学报(医学版), 2024, 56(4): 673-679. |
| [15] | 方杨毅,李强,黄志高,陆敏,洪锴,张树栋. 睾丸鞘膜高分化乳头状间皮肿瘤1例[J]. 北京大学学报(医学版), 2024, 56(4): 741-744. |
|
||
