北京大学学报(医学版) ›› 2023, Vol. 55 ›› Issue (6): 1013-1021. doi: 10.19723/j.issn.1671-167X.2023.06.009
艾拉莫德联合托法替布治疗难治性中重度类风湿关节炎的疗效
邹雪1,2,白小娟1,张丽卿1,*( )
)
- 1. 山西医科大学附属汾阳医院, 山西省汾阳医院风湿免疫科, 山西汾阳 032200
2. 苏州永鼎医院消化内科, 江苏苏州 215100
Effectiveness of tofacitinib combined with iguratimod in the treatment of difficult-to-treat moderate-to-severe rheumatoid arthritis
Xue ZOU1,2,Xiao-juan BAI1,Li-qing ZHANG1,*()
- 1. Department of Rheumatology and Immunology, Fenyang Hospital Affiliated to Shanxi Medical University, Shanxi Province Fenyang Hospital, Fenyang 032200, Shanxi, China
2. Department of Gastroenterology, Suzhou Yongding Hospital, Suzhou 215100, Jiangsu, China
摘要:
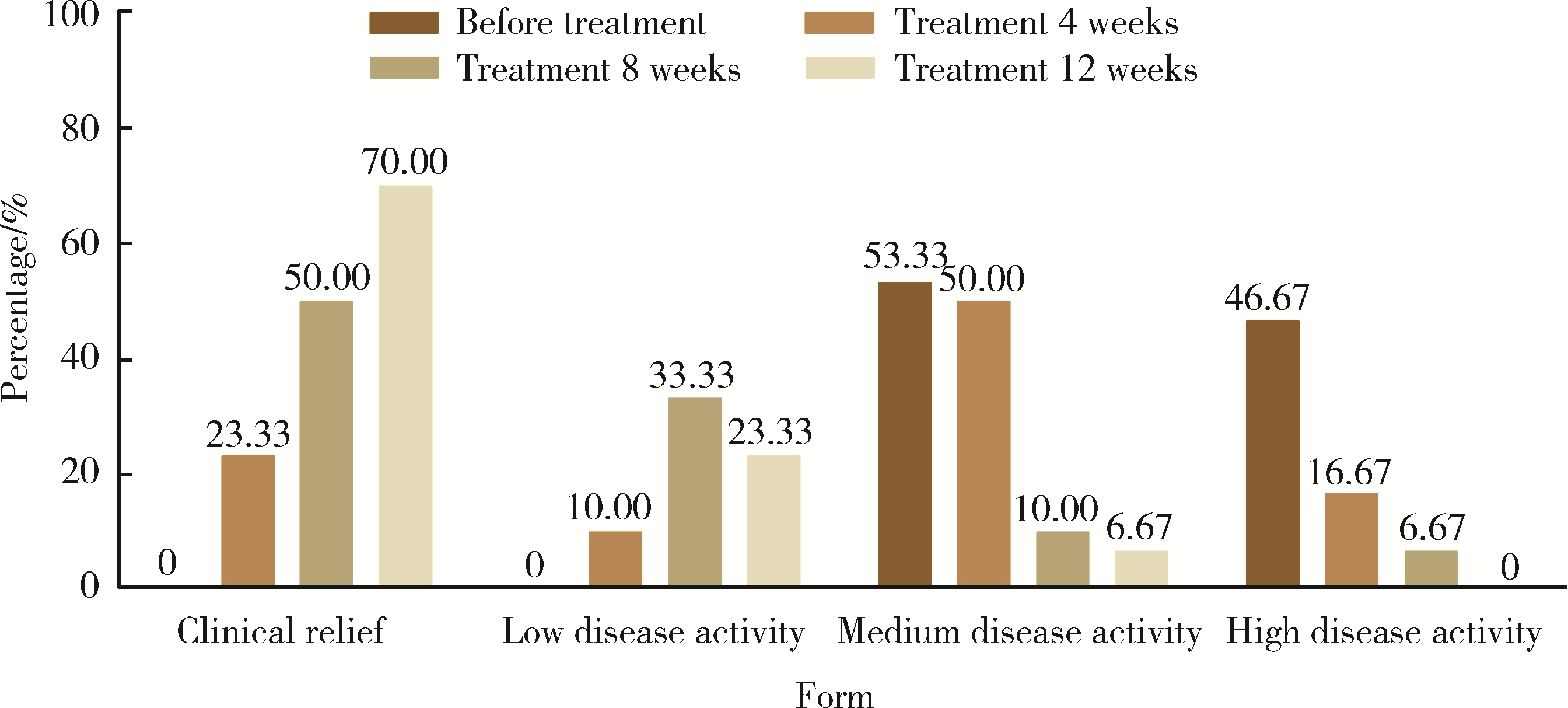
目的: 探讨艾拉莫德联合托法替布在难治性中重度类风湿关节炎(rheumatoid arthritis, RA)患者中的疗效和安全性。方法: 选择2021年9月至2022年6月规律就诊于山西省汾阳医院风湿免疫科的难治性中重度活动性RA患者30例进行前瞻性临床研究,其中,23例患者采用≥2种传统合成改善病情抗风湿药(disease modifying anti-rheumatic drugs,DMARDs)(至少包括甲氨蝶呤或来氟米特)治疗6个月以上,7例患者采用传统合成DMARDs联合肿瘤坏死因子拮抗剂治疗。将DMARDs调整为艾拉莫德联合托法替布,共治疗12周,收集患者治疗前,治疗4周、8周及12周时的临床资料:肿胀关节数(swollen joints count,SJC)、疼痛关节数(tender joints count,TJC)、晨僵时间、临床疾病活动指数(clinical disease activity index,CDAI)、健康状况评估问卷(health status assessment questionnaire,HAQ)、28个关节计数的疾病活动评分(28-joint disease activity score,DAS28)。记录患者的红细胞沉降率(erythrocyte sedimentation rate, ESR)、C反应蛋白(C-reactive protein, CRP)、血小板(platelet, PLT)、类风湿因子(rheumatoid factor, RF)、球蛋白、抗环瓜氨酸肽(cyclic citrullinated peptide, CCP)抗体等实验室检查结果,记录患者的用药情况,比较患者疾病活动指标的变化情况,记录药物不良反应。结果: 比较治疗前后的ESR、CRP、RF、PLT、SJC、TJC、基于ESR的DAS28(DAS28-ESR)、晨僵时间、HAQ、CDAI、抗CCP抗体,差异均有统计学意义(P < 0.05),而治疗前后的球蛋白比较差异无统计学意义(P>0.05)。艾拉莫德联合托法替布治疗期间,所有患者均未发生白细胞减少、肝酶明显升高、过敏、血栓栓塞等严重不良反应。结论: 艾拉莫德联合托法替布治疗难治性中重度RA,可通过降低炎性指标改善患者的近期临床症状,且安全性良好。
中图分类号:
- R593.22

| 1 |
Smolen JS , Landewé RBM , Bijlsma JWJ , et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying anti-rheumatic drugs: 2019 update[J]. Ann Rheum Dis, 2020, 79 (6): 685- 699.
doi: 10.1136/annrheumdis-2019-216655 |
| 2 | de Hair MJH , Jacobs JWG , Schoneveld JLM , et al. Difficult-to-treat rheumatoid arthritis: An area of unmet clinical need[J]. Rheumatology (Oxford), 2018, 57 (7): 1135- 1144. |
| 3 |
Buch MH . Defining refractory rheumatoid arthritis[J]. Ann Rheum Dis, 2018, 77 (7): 966- 969.
doi: 10.1136/annrheumdis-2017-212862 |
| 4 |
Smolen JS , Aletaha D , Mcinnes IB . Rheumatoid arthritis[J]. Lancet, 2016, 388 (10055): 2023- 2038.
doi: 10.1016/S0140-6736(16)30173-8 |
| 5 |
Aletaha D , Neogi T , Silman AJ , et al. 2010 rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism Collaborative initiative[J]. Arthritis Rheum, 2010, 62 (9): 2569- 2581.
doi: 10.1002/art.27584 |
| 6 |
Wu D , Luo Y , Li T , et al. Systemic complications of rheumatoid arthritis: Focus on pathogenesis and treatment[J]. Front Immunol, 2022, 13, 1051082.
doi: 10.3389/fimmu.2022.1051082 |
| 7 |
Sun X , Li R , Cai Y , et al. Clinical remission of rheumatoid arthritis in a multi center real-world study in Asia-Pacific region[J]. Lancet Reg Health West Pac, 2021, 15, 100240.
doi: 10.1016/j.lanwpc.2021.100240 |
| 8 | 李宏超, 徐丽玲, 苏茵. 难治性类风湿关节炎诊治探讨[J]. 中华风湿病学杂志, 2019, 23 (10): 689- 693. |
| 9 |
Nagy G , Roodenrijs NMT , Welsing PM , et al. EULAR definition of difficult-to-treat rheumatoid arthritis[J]. Ann Rheum Dis, 2021, 80 (1): 31- 35.
doi: 10.1136/annrheumdis-2020-217344 |
| 10 |
Xie S , Li S , Tian J , et al. Iguratimod as a new drug for rheumatoid arthritis: Current landscape[J]. Front Pharmacol, 2020, 11, 73.
doi: 10.3389/fphar.2020.00073 |
| 11 | Xu Y , Zhu Q , Song J , et al. Regulatory effect of iguratimod on the balance of Th subsets and inhibition of inflammatory cytokines in patients with rheumatoid arthritis[J]. Mediators Inflamm, 2015, 2015, 356040. |
| 12 | Wen L , Jiang W , Zhou M , et al. Effect of combined application of iguratimod in the treatment of active rheumatoid arthritis on bone metabolism, Th17 cells and Treg cells[J]. Am J Transl Res, 2021, 13 (3): 1676- 1684. |
| 13 |
Liu S , Song LP , Li RB , et al. Iguratimod promotes transformation of mononuclear macrophages in elderly patients with rheumatoid arthritis by nuclear factor-κB pathway[J]. World J Clin Cases, 2021, 9 (10): 2181- 2191.
doi: 10.12998/wjcc.v9.i10.2181 |
| 14 |
Li CH , Ma ZZ , Jian LL , et al. Iguratimod inhibits osteoclastoge-nesis by modulating the RANKL and TNF-α signaling pathways[J]. Int Immunopharmacol, 2021, 90, 107219.
doi: 10.1016/j.intimp.2020.107219 |
| 15 |
Kondo N , Kuroda T , Kobayashi D . Cytokine networks in the pa-thogenesis of rheumatoid arthritis[J]. Int J Mol Sci, 2021, 22 (20): 10922.
doi: 10.3390/ijms222010922 |
| 16 | Malemud CJ . The role of the JAK/STAT signal pathway in rheumatoid arthritis[J]. Ther Adv Musculoskelet Dis, 2018, 10 (5/6): 117- 127. |
| 17 | 疏金玲, 张玲玲, 魏伟. 酪氨酸激酶抑制剂治疗类风湿关节炎研究进展[J]. 中国药理学与毒理学杂志, 2020, 34 (9): 713- 720. |
| 18 |
Puigdevall L , Michiels C , Stewardson C , et al. JAK/STAT: Why choose a classical or an alternative pathway when you can have both?[J]. J Cell Mol Med, 2022, 26 (7): 1865- 1875.
doi: 10.1111/jcmm.17168 |
| 19 | 戴冰冰, 刘佳丽, 李宁宁, 等. 托法替布治疗难治性中重度类风湿关节炎的疗效及安全性[J]. 实用临床医药杂志, 2022, 26 (11): 122- 126. |
| 20 |
Zheng N , Guo C , Wu R . Iguratimod is effective in refractory rheumatoid arthritis patients with inadequate response to metho-trexate-cyclosporin A-hydroxychloroquine-prednisone[J]. Scand J Rheumatol, 2018, 47 (5): 422- 424.
doi: 10.1080/03009742.2017.1376109 |
| 21 |
Mizutani S , Kodera H , Sato Y , et al. Clinical effectiveness of iguratimod based on real-world data of patients with rheumatoid arthritis[J]. Clin Rheumatol, 2021, 40 (1): 123- 132.
doi: 10.1007/s10067-020-05208-y |
| 22 | Inoue A , Nozaki Y , Hirooka Y , et al. The effectiveness and retention rate of iguratimod in Japanese rheumatoid arthritis patients with/without methotrexate in daily medical care[J]. Life (Basel), 2020, 10 (11): 261. |
| 23 | Ouyang D , Ma YZ , Zou J , et al. Effectiveness and safety of iguratimod monotherapy or combined with methotrexate in treating rheumatoid arthritis: A aystematic review and meta-analysis[J]. Front Pharmacol, 2022, 13, 911810. |
| 24 | Smolen JS , Landewe R , Breedveld FC , et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2013 update[J]. Ann Rheum Dis, 2014, 73 (3): 492- 509. |
| 25 | Angelini J , Talotta R , Roncato R , et al. JAK-inhibitors for the treatment of rheumatoid arthritis: A focus on the present and an outlook on the future[J]. Biomolecules, 2020, 10 (7): 1002. |
| 26 | 张春燕, 范小冬, 秦元, 等. JAK抑制剂托法替布治疗类风湿性关节炎效果的Meta分析[J]. 第三军医大学学报, 2018, 40 (6): 543- 550. |
| 27 | Sands BE , Taub PR , Armuzzi A , et al. Tofacitinib treatment is associated with modest and reversible increases in serum lipids in patients with ulcerative colitis[J]. Clin Gastroenterol Hepatol, 2020, 18 (1): 123- 132.e3. |
| 28 | Taylor PC , Kremer JM , Emery P , et al. Lipid profile and effect of statin treatment in pooled phase Ⅱ and phase Ⅲ baricitinib studies[J]. Ann Rheum Dis, 2018, 77 (7): 988- 995. |
| [1] | 步召德, 冯梦宇, 季科. 早期胃癌行前哨淋巴结导航手术的实践与思考[J]. 北京大学学报(医学版), 2026, 58(2): 239-243. |
| [2] | 魏慧, 张警丰, 姚中强, 赵金霞. 类风湿关节炎合并慢性病贫血患者的临床特征及相关因素[J]. 北京大学学报(医学版), 2026, 58(2): 307-312. |
| [3] | 李伟浩, 张学民, 李伟, 张韬, 张小明. 胸主动脉腔内修复术左肱动脉穿刺点使用血管缝合器处理的临床效果[J]. 北京大学学报(医学版), 2026, 58(2): 388-392. |
| [4] | FarinEbrahimi, 冯志强, FarazEbrahimi, 韩玮华, 于子杨, 贾宽宽, 安金刚. 上颌药物相关性颌骨坏死的不同分期手术治疗效果[J]. 北京大学学报(医学版), 2026, 58(1): 107-114. |
| [5] | 潘莲菲, 李文静, 王瑞洋, 焦剑, 曹战强, 高丽, 释栋. 口服抗生素辅助牙周机械治疗对重度牙周炎的短期疗效及影响因素[J]. 北京大学学报(医学版), 2026, 58(1): 30-36. |
| [6] | 吴滔, 林建子, 朱亚锋, 马剑达, 贾霈雯, 杨莉娟, 潘婕, 邹耀威, 杨迎, 卢烨, 戴冽. 血清蛋白质谱筛选及验证类风湿关节炎患者肌肉量减少的生物标志物[J]. 北京大学学报(医学版), 2025, 57(6): 1024-1031. |
| [7] | 丁艳, 王丽芳, 李超然, 卢哲敏, 石连杰. 利妥昔单抗成功治疗类风湿关节炎合并IgG4相关性疾病1例[J]. 北京大学学报(医学版), 2025, 57(6): 1203-1207. |
| [8] | 杨菊, 徐婧, 戴菊华, 石连杰. Lumican蛋白在类风湿关节炎患者血清中的表达及其与疾病和免疫活动的相关性[J]. 北京大学学报(医学版), 2025, 57(5): 911-918. |
| [9] | 冯亮华, 洪丽荣, 陈雨佳, 蔡学明. 泛素特异性蛋白酶35对类风湿关节炎成纤维样滑膜细胞铁死亡的作用及机制[J]. 北京大学学报(医学版), 2025, 57(5): 919-925. |
| [10] | 康一帆, 葛严军, 吕晓鸣, 谢尚, 单小峰, 蔡志刚. 即刻种植体支持式义齿修复的血管化髂骨瓣重建下颌骨缺损[J]. 北京大学学报(医学版), 2025, 57(1): 78-84. |
| [11] | 贾霈雯, 杨迎, 邹耀威, 欧阳志明, 林建子, 马剑达, 杨葵敏, 戴冽. 类风湿关节炎患者低肌肉量综合征的临床特征及其对躯体功能的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1009-1016. |
| [12] | 马豆豆, 卢哲敏, 郭倩, 朱莎, 古今, 丁艳, 石连杰. 小剂量利妥昔单抗成功治疗类风湿关节炎合并重症肌无力1例[J]. 北京大学学报(医学版), 2024, 56(6): 1110-1114. |
| [13] | 闫蕊, 柯丹, 张妍, 李丽, 苏焕然, 陈伟, 孙明霞, 刘晓敏, 罗靓. 血清趋化因子CXCL-10和涎液化糖链抗原6水平在类风湿关节炎合并肺间质病变患者中的诊断和病情评估价值[J]. 北京大学学报(医学版), 2024, 56(6): 956-962. |
| [14] | 赵亮, 史成龙, 马柯, 赵静, 王潇, 邢晓燕, 莫万星, 练益瑞, 高超, 李玉慧. 抗合成酶综合征重叠类风湿关节炎患者的免疫学特征[J]. 北京大学学报(医学版), 2024, 56(6): 972-979. |
| [15] | 韩艺钧, 陈小莉, 李常虹, 赵金霞. 甲氨蝶呤在类风湿关节炎患者中的应用现状[J]. 北京大学学报(医学版), 2024, 56(6): 994-1000. |
|
||
