北京大学学报(医学版) ›› 2026, Vol. 58 ›› Issue (3): 631-640. doi: 10.19723/j.issn.1671-167X.2026.03.025
预后不良的肾细胞癌伴淋巴结转移的分子特征
舒帆1,2,*, 葛力源1,*, 邓汉彰1,3, 殷昊明1, 欧俊永1, 邓绍晖1, 郝一昌1, 陆敏4,5, 张展奕1, 段佩辰1, 张树栋1,*( )
)
- 1. 北京大学第三医院泌尿外科, 北京 100191
2. 昆明医科大学第二附属医院泌尿外科, 昆明 650101
3. 北京协和医院生物标志物研究平台, 北京 100730
4. 北京大学第三医院病理科, 北京 100191
5. 北京大学基础医学院病理学系, 北京 100191
Molecular characteristics for poor prognosis related renal cell carcinoma with lymph metastases
Fan SHU1,2, Liyuan GE1, Hanzhang DENG1,3, Haoming YIN1, Junyong OU1, Shaohui DENG1, Yichang HAO1, Min LU4,5, Zhanyi ZHANG1, Peichen DUAN1, Shudong ZHANG1,*()
- 1. Department of Urology, Peking University Third Hospital, Beijing 100191, China
2. Department of Urology, The Second Affiliated Hospital of Kunming Medical University, Kunming 650101, China
3. Center for Biomarker Discovery and Validation, National Infrastructures for Translation Medicine, Institute of Clinical Medicine, Peking Union Medical College Hospital, Beijing 100730, China
4. Department of Pathology, Peking University Third Hospital, Beijing 100191, China
5. Department of Pathology, Peking University School of Basic Medical Sciences, Beijing 100191, China
摘要:
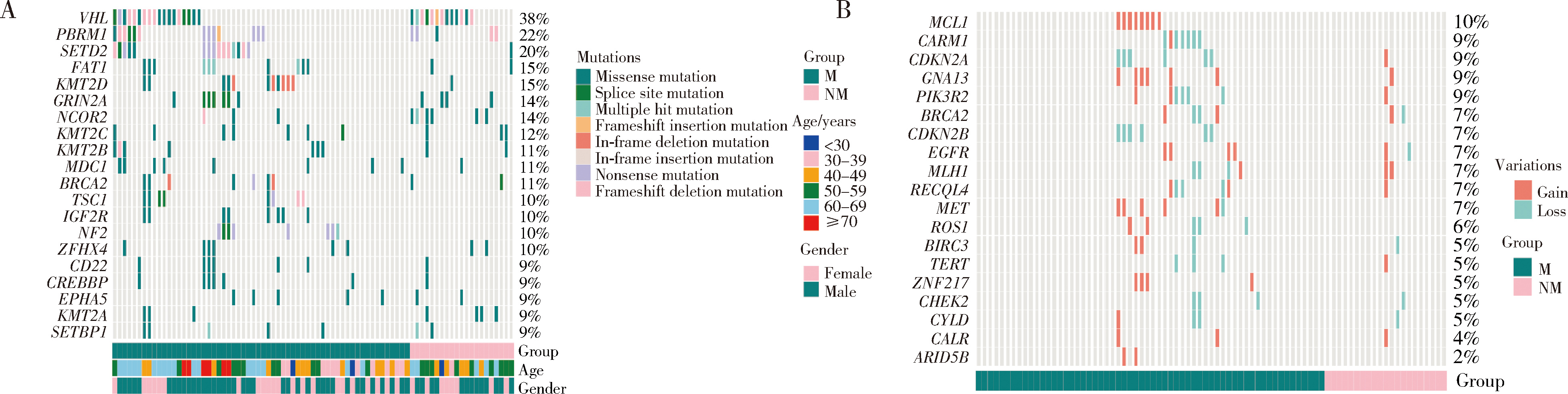
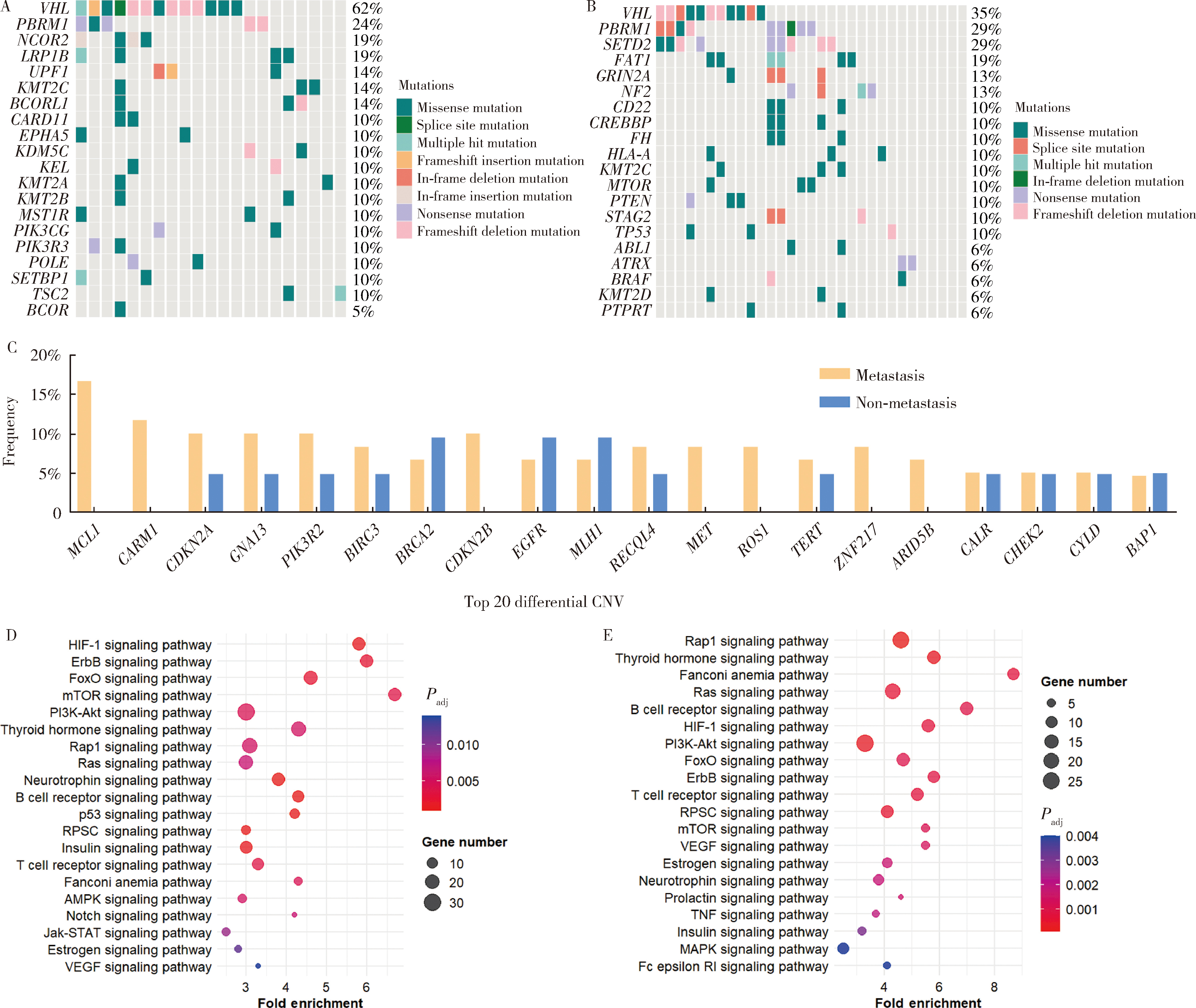
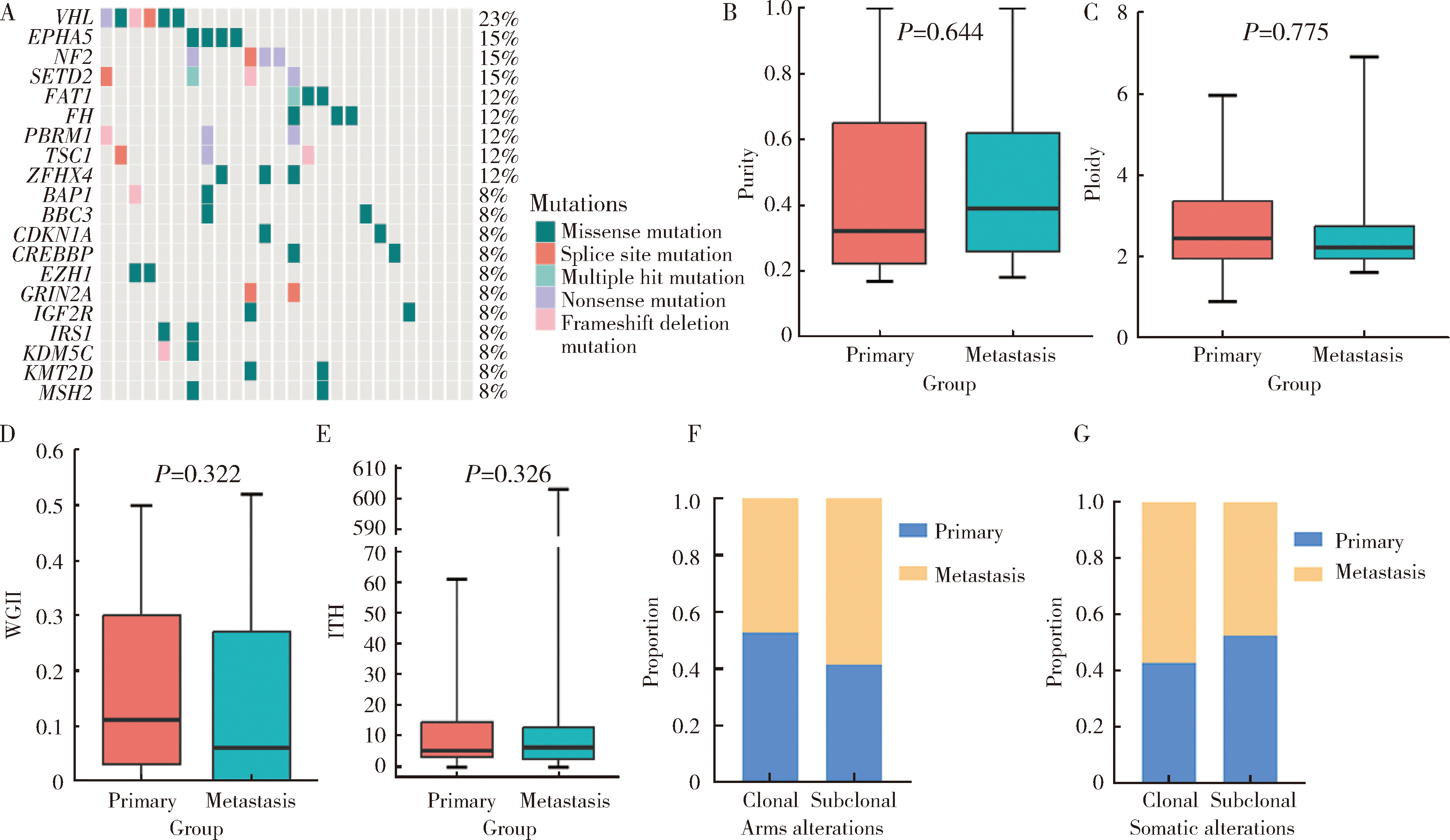
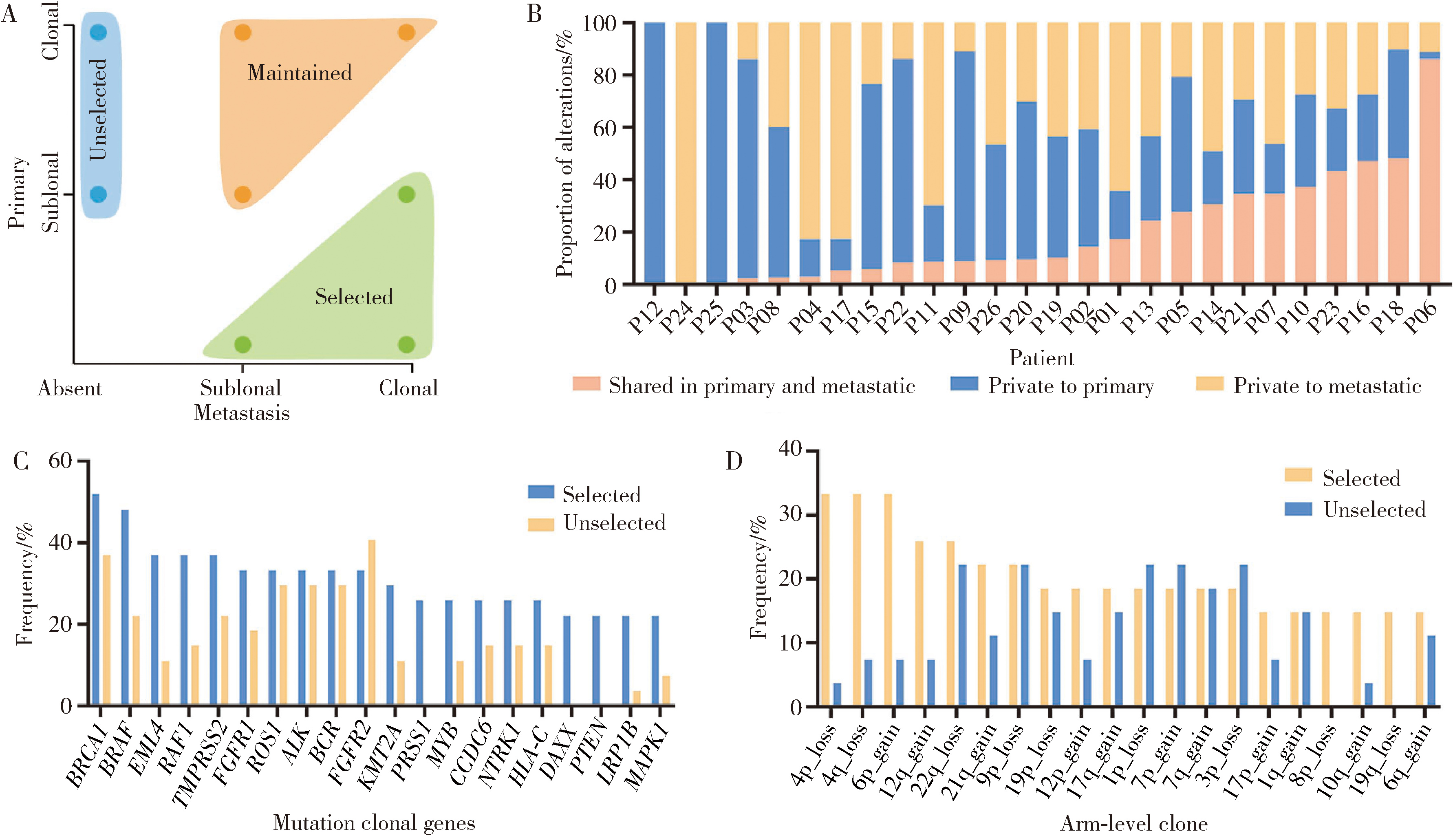
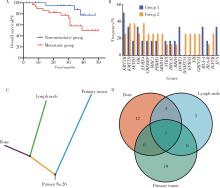
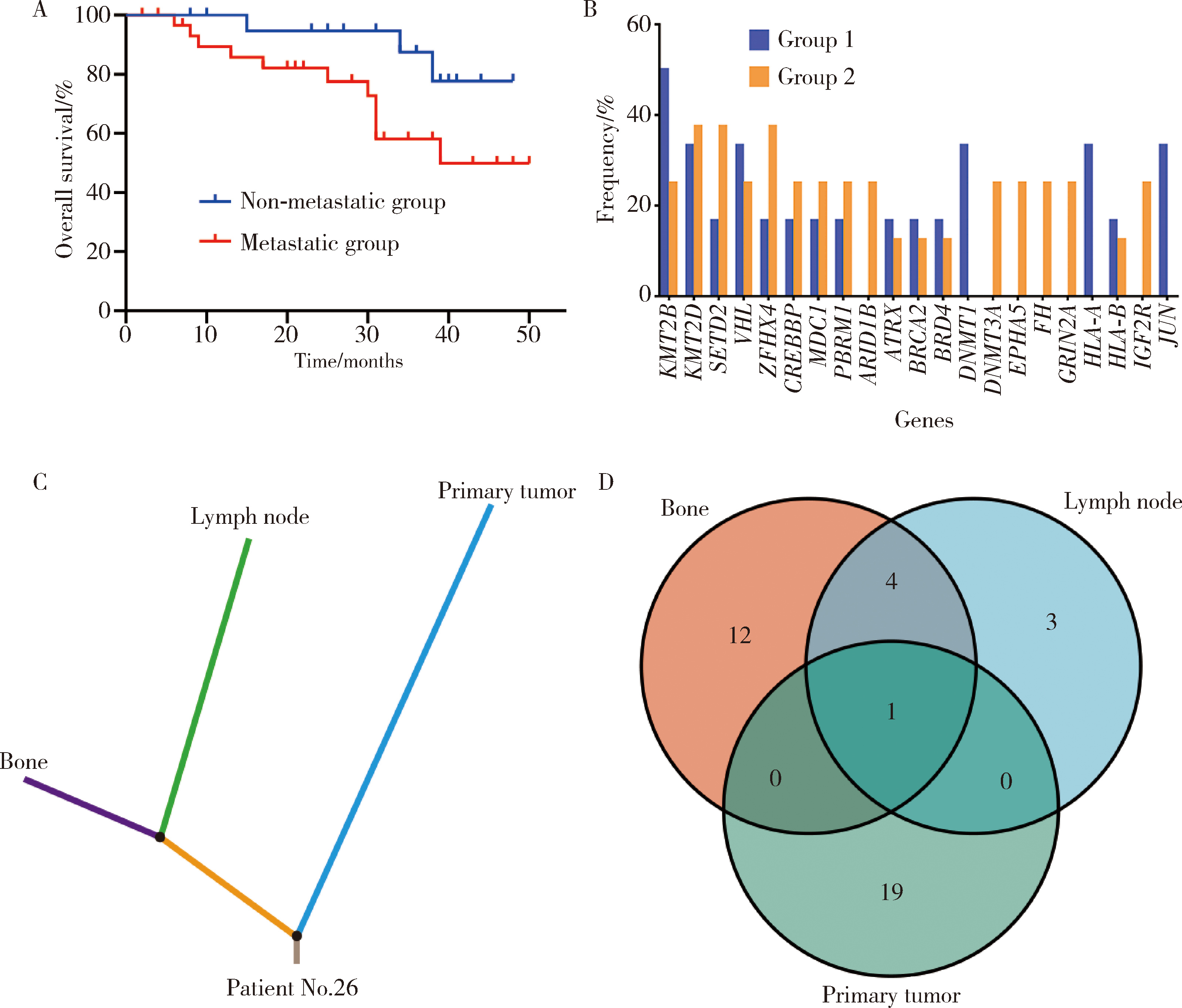
目的: 通过下一代测序(next-generation sequencing,NGS)技术分析肾细胞癌(简称肾癌)淋巴结转移的基因突变谱,发现与预后不良相关的分子特征,为肾癌机制的研究以及治疗提供新的思路。方法: 对31例淋巴结转移的肾癌和21例非转移性肾癌患者的临床资料进行回顾性分析,同时从病理科调取肿瘤原发灶、淋巴结转移灶、远处转移灶的石蜡包埋组织共81例,使用NGS技术检测患者的基因突变谱,术后随访分析淋巴结转移与患者预后的关系。结果: 与非转移性肾癌相比,淋巴结转移肾癌在肿瘤大小(P=0.006)、世界卫生组织(World Health Organization,WHO)/国际泌尿病理协会(International Society of Urological Pathology, ISUP)分级(P=0.002)、T分期(P=0.003)、合并癌栓(P=0.025)上差异有统计学意义。最常见的突变基因是肿瘤抑制基因VHL (38%)、PBRM1 (22%)和IGF2R (20%),且拷贝数变异与肿瘤转移相关,部分突变特征与已知的突变模式高度相似。淋巴结转移组和非转移组患者的突变频率存在差异,转移组大多数基因的突变频率较高,然而Reactome通路富集分析未在两组共有的富集途径上显示出差异有统计学意义。同一患者的肿瘤原发灶和转移灶之间有很强的一致性,基因组学指标[如纯度、倍性、加权基因组完整性指数(weighted-genomic integrity index, WGII)和肿瘤内异质性(intra-tumor heterogeneity, ITH)]及克隆、亚克隆组成分析进一步支持了这种一致性。无转移组的总生存率较高(P=0.041),且特定基因突变(如IGF2R、JUN、EPHA5和FH)与较差的预后相关。淋巴结可能起到“转移池”的作用,促进肾癌的远处转移。结论: 多基因NGS同时评估了多个相关标记物,揭示了淋巴结转移肾癌患者的基因改变谱,基于NGS的分子分析可以帮助临床医生评估患者的预后,并发现新的机制及治疗靶点。
中图分类号:
- R737.11




| 1 |
|
| 2 |
doi: 10.1016/S0140-6736(15)00046-X |
| 3 |
doi: 10.1001/jamanetworkopen.2020.21869 |
| 4 |
doi: 10.1056/NEJMra043172 |
| 5 |
doi: 10.1016/j.eururo.2011.09.003 |
| 6 |
doi: 10.7717/peerj.12493 |
| 7 |
doi: 10.1152/ajprenal.00138.2016 |
| 8 |
doi: 10.1016/j.cell.2018.03.057 |
| 9 |
doi: 10.1016/j.euf.2017.09.016 |
| 10 |
doi: 10.1038/ng.3146 |
| 11 |
doi: 10.1016/j.celrep.2016.02.024 |
| 12 |
doi: 10.1038/s41416-018-0064-3 |
| 13 |
doi: 10.3389/fonc.2022.851552 |
| 14 |
|
| 15 |
doi: 10.1016/j.semcancer.2020.05.010 |
| 16 |
doi: 10.1007/s13402-020-00526-4 |
| 17 |
doi: 10.18632/oncotarget.14966 |
| 18 |
|
| 19 |
doi: 10.1002/ddr.21967 |
| 20 |
doi: 10.7150/jca.57711 |
| 21 |
doi: 10.1111/apm.13222 |
| 22 |
|
| 23 |
doi: 10.1186/s12935-020-1101-x |
| 24 |
doi: 10.1038/ng849 |
| 25 |
doi: 10.1080/14728222.2020.1804862 |
| 26 |
|
| 27 |
|
| 28 |
|
| 29 |
|
| 30 |
|
| 31 |
|
| 32 |
|
| 33 |
|
| [1] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [2] | 张铃福, 陈明, 赵小宇, 王港, 崔龙, 凌晓锋, 王立新, 徐智, 郭丽梅, 侯纯升. 原发灶局限于胆囊壁内胆囊癌大体分型及其与预后和癌前病变的相关性[J]. 北京大学学报(医学版), 2026, 58(1): 184-189. |
| [3] | 高雅静, 李正芳, 马梦思, 武丽君. SII和SIRI对白塞病葡萄膜炎的风险预测及疾病活动度和预后的评估[J]. 北京大学学报(医学版), 2025, 57(6): 1067-1073. |
| [4] | 郭博达, 陆敏, 王国良, 张洪宪, 刘磊, 侯小飞, 赵磊, 田晓军, 张树栋. 肾透明细胞癌与非透明细胞癌伴静脉癌栓患者的临床病理特征及预后比较[J]. 北京大学学报(医学版), 2025, 57(4): 644-649. |
| [5] | 张展奕, 陆敏, 孙悦皓, 董靖晗, 侯小飞, 肖春雷, 王国良, 田晓军, 马潞林, 张洪宪, 张树栋. TFE3重排肾细胞癌合并静脉癌栓患者的临床病理特征及生存分析[J]. 北京大学学报(医学版), 2025, 57(4): 650-661. |
| [6] | 王泽远, 于栓宝, 郑浩轲, 陶金, 范雅峰, 张雪培. 基于临床特征和多参数MRI的前列腺癌盆腔淋巴结转移的术前预测模型[J]. 北京大学学报(医学版), 2025, 57(4): 684-691. |
| [7] | 周泽臻, 葛力源, 张帆, 邓绍晖, 颜野, 张洪宪, 王国良, 刘磊, 黄毅, 张树栋. 病理T3a期肾细胞癌肾部分切除与根治性肾切除的回顾性匹配研究[J]. 北京大学学报(医学版), 2025, 57(4): 704-710. |
| [8] | 李伟浩, 李晶, 张学民, 李伟, 李清乐, 张小明. 术中回收式自体输血对颈动脉体瘤切除术后肿瘤预后的影响[J]. 北京大学学报(医学版), 2025, 57(2): 272-276. |
| [9] | 毛雅晴, 陈震, 于尧, 章文博, 刘洋, 彭歆. 2型糖尿病对口腔鳞状细胞癌患者预后的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1089-1096. |
| [10] | 欧俊永,倪坤明,马潞林,王国良,颜野,杨斌,李庚午,宋昊东,陆敏,叶剑飞,张树栋. 肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素[J]. 北京大学学报(医学版), 2024, 56(4): 582-588. |
| [11] | 刘帅,刘磊,刘茁,张帆,马潞林,田晓军,侯小飞,王国良,赵磊,张树栋. 伴静脉癌栓的肾上腺皮质癌的临床治疗及预后[J]. 北京大学学报(医学版), 2024, 56(4): 624-630. |
| [12] | 虞乐,邓绍晖,张帆,颜野,叶剑飞,张树栋. 具有低度恶性潜能的多房囊性肾肿瘤的临床病理特征及预后[J]. 北京大学学报(医学版), 2024, 56(4): 661-666. |
| [13] | 周泽臻,邓绍晖,颜野,张帆,郝一昌,葛力源,张洪宪,王国良,张树栋. 非转移性T3a肾细胞癌患者3年肿瘤特异性生存期预测[J]. 北京大学学报(医学版), 2024, 56(4): 673-679. |
| [14] | 方杨毅,李强,黄志高,陆敏,洪锴,张树栋. 睾丸鞘膜高分化乳头状间皮肿瘤1例[J]. 北京大学学报(医学版), 2024, 56(4): 741-744. |
| [15] | 曾媛媛,谢云,陈道南,王瑞兰. 脓毒症患者发生正常甲状腺性病态综合征的相关因素[J]. 北京大学学报(医学版), 2024, 56(3): 526-532. |
|
||
