北京大学学报(医学版) ›› 2023, Vol. 55 ›› Issue (2): 243-253. doi: 10.19723/j.issn.1671-167X.2023.02.007
人表皮生长因子受体2低表达乳腺癌的临床病理学特征及预后
朱晓娟1,张虹1,*( ),张爽1,李东1,李鑫1,徐玲2,李挺1
),张爽1,李东1,李鑫1,徐玲2,李挺1
- 1. 北京大学第一医院病理科,北京 100034
2. 北京大学第一医院乳腺疾病中心,北京 100034
Clinicopathological features and prognosis of breast cancer with human epidermal growth factor receptor 2 low expression
Xiao-juan ZHU1,Hong ZHANG1,*(),Shuang ZHANG1,Dong LI1,Xin LI1,Ling XU2,Ting LI1
- 1. Department of Pathology, Peking University First Hospital, Beijing 100034, China
2. Breast Disease Center, Peking University First Hospital, Beijing 100034, China
摘要:
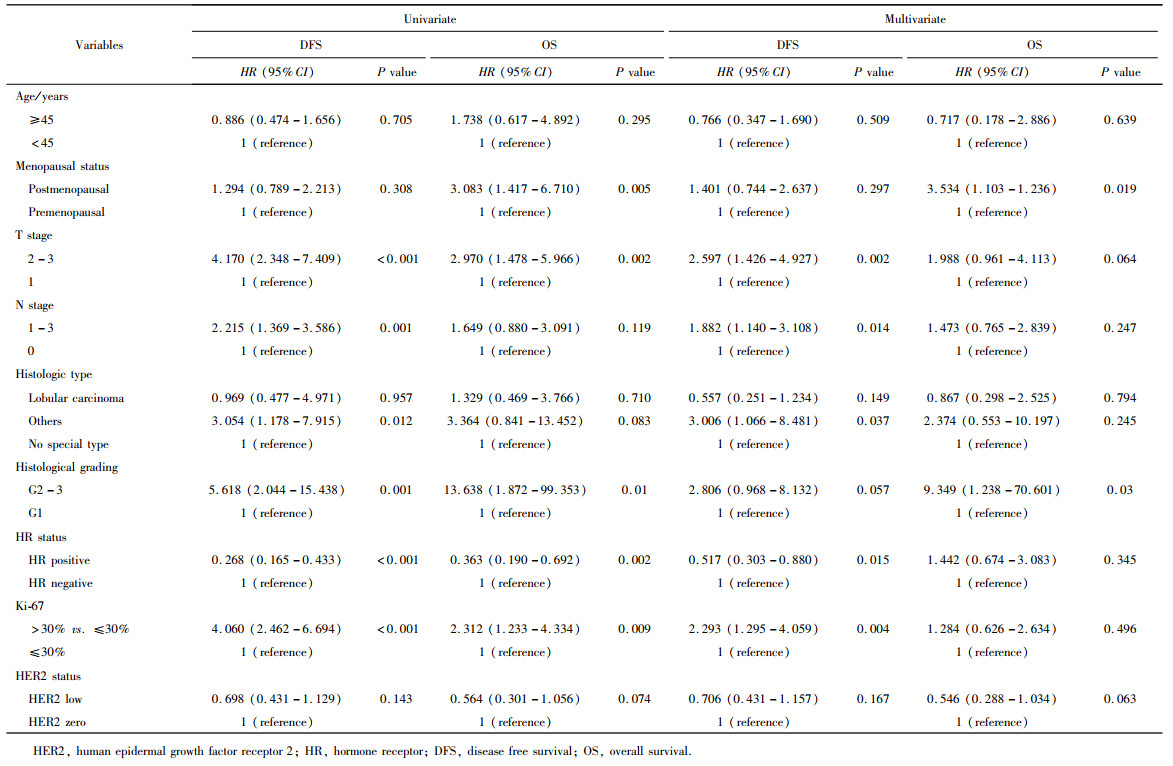
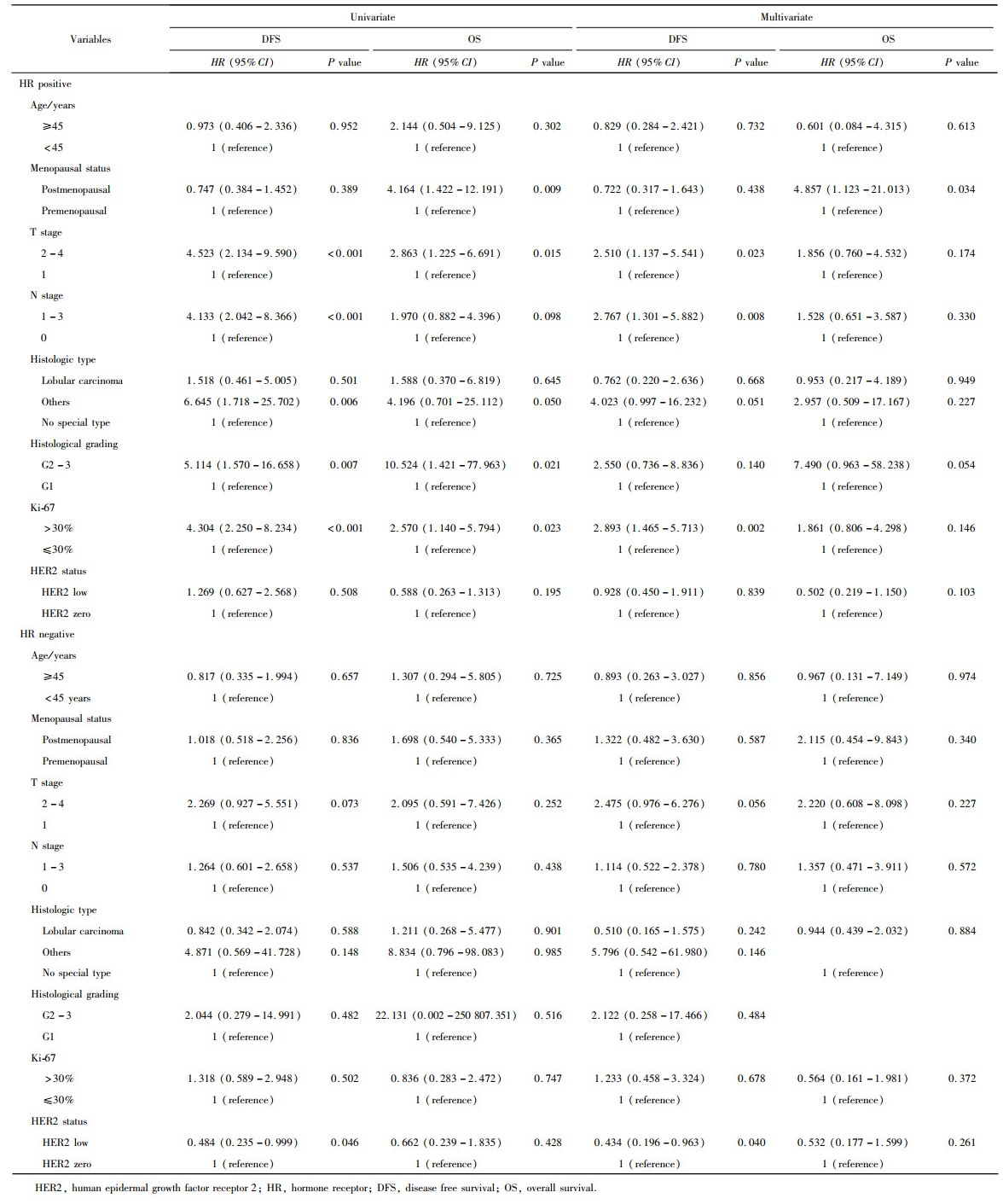
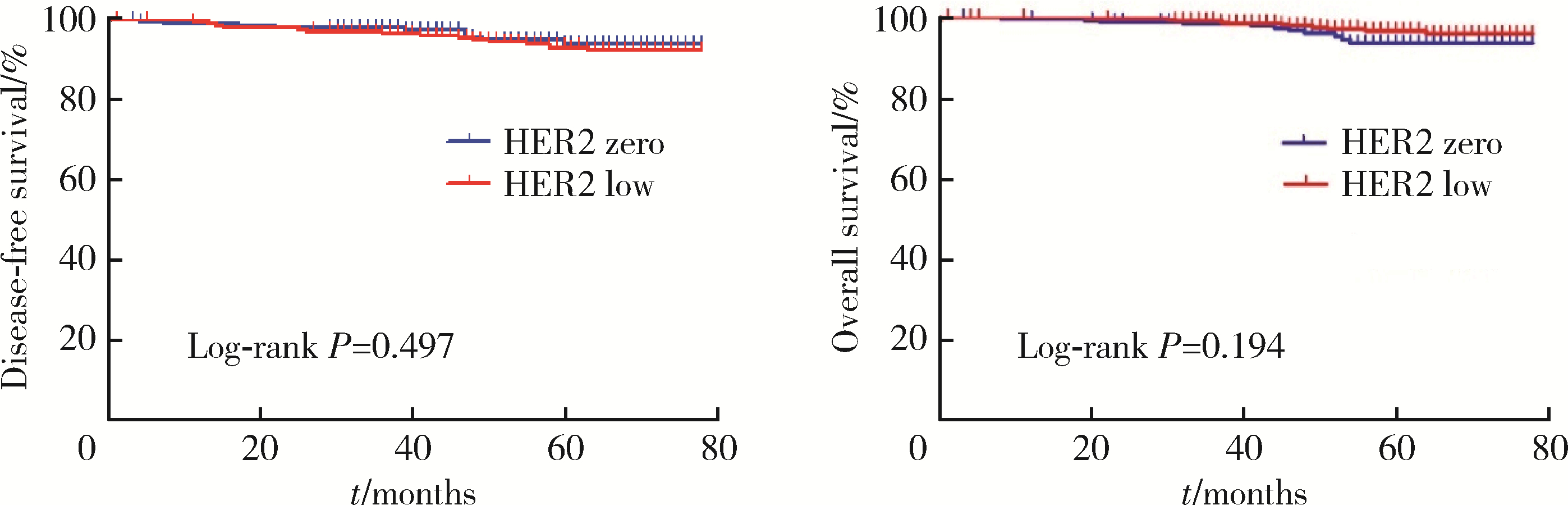
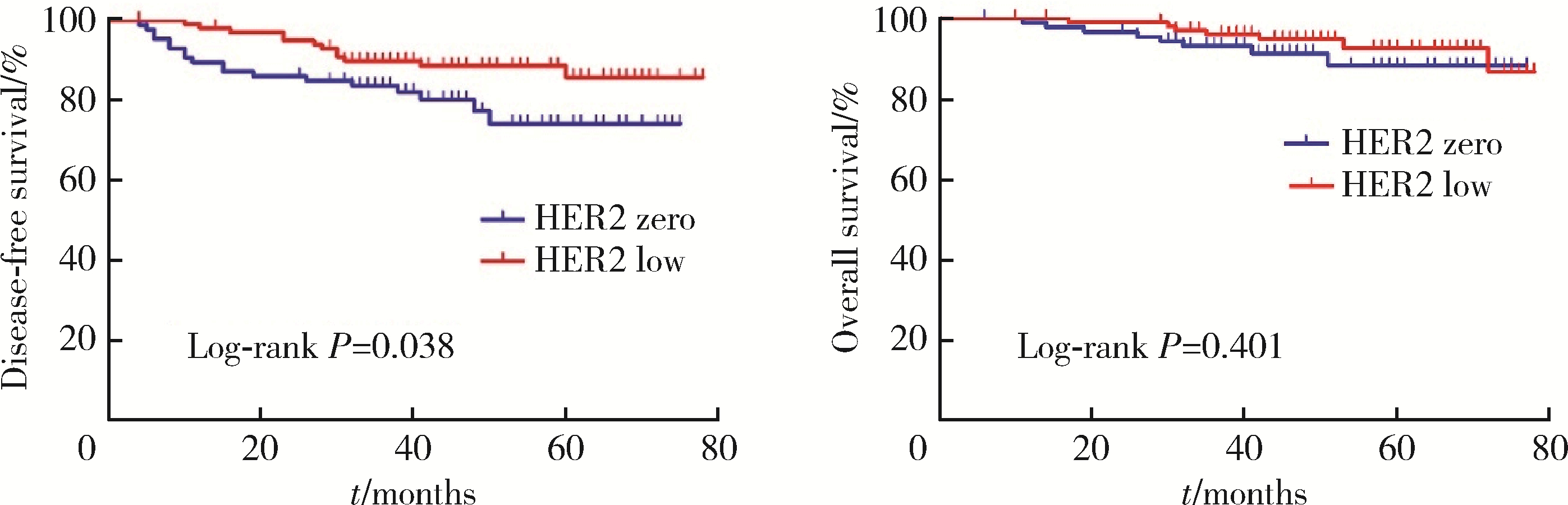
目的: 新型抗人表皮生长因子受体2(human epidermal growth factor receptor 2, HER2)抗体偶联药物临床试验的成功, 使HER2低表达乳腺癌是否将成为新的乳腺癌类型而受到关注。本研究分析比较HER2低表达与HER2零表达两组乳腺癌患者间的临床病理特征及生存数据, 探讨其临床生物学上的差异性。方法: 2014年1月至2017年12月北京大学第一医院乳腺疾病中心收治的1 250例女性原发性非转移性乳腺癌中, 969例HER2阴性(免疫组织化学染色评分为0、1+、2+, 且荧光原位杂交未扩增), 分析其中HER2低表达(1+或2+且荧光原位杂交未扩增)和HER2零表达(0分)两组患者间临床病理特征及预后情况。对两组患者进行无病生存期(disease free survival, DFS)和总生存期(overall survival, OS)预后评价, 采用Kaplan-Meier曲线计算生存率, Log-rank检验比较生存差异, 单因素和多因素Cox回归分析预后影响因素。采用双侧检验, P < 0.05为差异有统计学意义。结果: 969例HER2阴性乳腺癌中, HER2低表达者606例(62.54%)、HER2零表达者363例(37.46%)。与HER2零表达组相比, HER2低表达组的N分期(P=0.001)和TNM分期更高(P=0.044), 非特殊型组织学类型占比(82.7% vs. 79.1%, P=0.009)和组织学分级更高(P=0.048), 激素受体阳性率偏高(83.2% vs. 75.2%, P=0.003), Ki-67增殖指数>30%者的比例偏低(30.4% vs. 36.6%, P=0.044)。两组间DFS及OS差异无统计学意义(P>0.05)。969例患者中, 激素受体阳性777例, 激素受体阴性(即三阴性乳腺癌)192例。激素受体阳性的777例中, HER2低表达504例(64.9%), HER2零表达273例(35.1%), 两组比较, HER2低表达组的发病年龄小(P=0.016), 未绝经者占比高(P=0.029), 淋巴结受累更多(P=0.002), TNM分期更高(P=0.031), 小叶癌和黏液癌组织学类型较少见(3.6% vs. 7.3%, 4.8% vs. 10.6%, P < 0.001), DFS和OS差异无统计学意义(P>0.05)。192例激素受体阴性(三阴性乳腺癌)中, HER2低表达102例(53.1%), HER2零表达90例(46.9%), 两组比较, HER2低表达组的发病年龄大(P=0.001), 未绝经所占比例低(P=0.029), 组织学分级更低(P < 0.001), Ki-67增殖指数更低(P < 0.001), 雄激素受体阳性率高(58.8% vs. 34.4%, P < 0.001), DFS比较好(P=0.038), OS差异无统计学意义(P>0.05)。结论: HER2低表达乳腺癌占所有乳腺癌约一半的比例, 发病远高于HER2阳性乳腺癌, 其临床病理特征存在异质性, 激素受体表达状态对HER2低表达乳腺癌的临床生物学有影响。
中图分类号:
- R737.9




| 1 | Yarden Y . Biology of HER2 and its importance in breast cancer[J]. Oncology, 2001, 61 (Suppl 2): 1- 13. |
| 2 |
Choong GM , Cullen GD , O'Sullivan CC , et al. Evolving stan-dards of care and new challenges in the management of HER2-positive breast cancer[J]. CA Cancer J Clin, 2020, 70 (5): 355- 374.
doi: 10.3322/caac.21634 |
| 3 |
Swain SM , Baselga J , Kim SB , et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer[J]. N Engl J Med, 2015, 372 (8): 724- 734.
doi: 10.1056/NEJMoa1413513 |
| 4 |
Wolff AC , Hammond ME , Hicks DG , et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Patho-logists clinical practice guideline update[J]. J Clin Oncol, 2013, 31 (31): 3997- 4013.
doi: 10.1200/JCO.2013.50.9984 |
| 5 |
Gilcrease MZ , Woodward WA , Nicolas MM , et al. Even low-level HER2 expression may be associated with worse outcome in node-positive breast cancer[J]. Am J Surg Pathol, 2009, 33 (5): 759- 767.
doi: 10.1097/PAS.0b013e31819437f9 |
| 6 |
Modi S , Park H , Murthy RK , et al. Antitumor activity and safety of trastuzumab deruxtecan in patients with HER2-low-expressing advanced breast cancer: Results from a phase Ⅰb study[J]. J Clin Oncol, 2020, 38 (17): 1887- 1896.
doi: 10.1200/JCO.19.02318 |
| 7 |
Tarantino P , Hamilton E , Tolaney SM , et al. HER2-low breast cancer: Pathological and clinical landscape[J]. J Clin Oncol, 2020, 38 (17): 1951- 1962.
doi: 10.1200/JCO.19.02488 |
| 8 |
Hammond ME , Hayes DF , Dowsett M , et al. American Society of Clinical Oncology/College Of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer[J]. J Clin Oncol, 2010, 28 (16): 2784- 2795.
doi: 10.1200/JCO.2009.25.6529 |
| 9 |
Schalper KA , Kumar S , Hui P , et al. A retrospective population-based comparison of HER2 immunohistochemistry and fluorescence in situ hybridization in breast carcinomas: Impact of 2007 American Society of Clinical Oncology/College of American Pathologists criteria[J]. Arch Pathol Lab Med, 2014, 138 (2): 213- 219.
doi: 10.5858/arpa.2012-0617-OA |
| 10 |
Xin L , Wu Q , Zhan C , et al. Multicenter study of the clinico-pathological features and recurrence risk prediction model of early-stage breast cancer with low-positive human epidermal growth factor receptor 2 expression in China (Chinese Society of Breast Surgery 021)[J]. Chin Med J (Engl), 2022, 135 (6): 697- 706.
doi: 10.1097/CM9.0000000000002056 |
| 11 |
Schettini F , Chic N , Brasó-Maristany F , et al. Clinical, patholo-gical, and PAM50 gene expression features of HER2-low breast cancer[J]. NPJ Breast Cancer, 2021, 7 (1): 1.
doi: 10.1038/s41523-020-00208-2 |
| 12 |
Denkert C , Seither F , Schneeweiss A , et al. Clinical and molecular characteristics of HER2-low-positive breast cancer: Pooled analysis of individual patient data from four prospective, neoadjuvant clinical trials[J]. Lancet Oncol, 2021, 22 (8): 1151- 1161.
doi: 10.1016/S1470-2045(21)00301-6 |
| 13 |
Rossi V , Sarotto I , Maggiorotto F , et al. Moderate immunohistochemical expression of HER-2 (2+) without HER-2 gene amplification is a negative prognostic factor in early breast cancer[J]. Oncologist, 2012, 17 (11): 1418- 1425.
doi: 10.1634/theoncologist.2012-0194 |
| 14 |
Won HS , Ahn J , Kim Y , et al. Clinical significance of HER2-low expression in early breast cancer: A nationwide study from the Korean Breast Cancer Society[J]. Breast Cancer Res, 2022, 24 (1): 22.
doi: 10.1186/s13058-022-01519-x |
| 15 |
Horisawa N , Adachi Y , Takatsuka D , et al. The frequency of low HER2 expression in breast cancer and a comparison of prognosis between patients with HER2-low and HER2-negative breast cancer by HR status[J]. Breast Cancer, 2022, 29 (2): 234- 241.
doi: 10.1007/s12282-021-01303-3 |
| 16 |
Dehghani M , Keshavarz P , Talei A , et al. The Effects of Low HER2/neu expression on the clinicopathological characteristics of triple-negative breast cancer patients[J]. Asian Pac J Cancer Prev, 2020, 21 (10): 3027- 3032.
doi: 10.31557/APJCP.2020.21.10.3027 |
| 17 |
Jacot W , Maran-Gonzalez A , Massol O , et al. Prognostic value of HER2-low expression in non-metastatic triple-negative breast cancer and correlation with other biomarkers[J]. Cancers (Basel), 2021, 13 (23): 6059.
doi: 10.3390/cancers13236059 |
| [1] | 彭博, 刘芳芳, 杨伟, 徐瑞平, 陈蕾, 李保中, 王新家, 柯骥, 杨文蕾, 何煜, 刘震, 侯波林, 张利群, 林妙萍, 张立新, 张凡, 蔡奋, 许铧文, 刘萌飞, 刘英, 潘雅琪, 何忠虎, 柯杨. 围术期高血糖与食管切除术后食管鳞癌不良预后相关性[J]. 北京大学学报(医学版), 2026, 58(3): 567-574. |
| [2] | 舒帆, 葛力源, 邓汉彰, 殷昊明, 欧俊永, 邓绍晖, 郝一昌, 陆敏, 张展奕, 段佩辰, 张树栋. 预后不良的肾细胞癌伴淋巴结转移的分子特征[J]. 北京大学学报(医学版), 2026, 58(3): 631-640. |
| [3] | 王海, 江一舟. 靶向血管治疗在乳腺癌精准治疗中的分子机制与临床应用[J]. 北京大学学报(医学版), 2026, 58(2): 251-256. |
| [4] | 张铃福, 陈明, 赵小宇, 王港, 崔龙, 凌晓锋, 王立新, 徐智, 郭丽梅, 侯纯升. 原发灶局限于胆囊壁内胆囊癌大体分型及其与预后和癌前病变的相关性[J]. 北京大学学报(医学版), 2026, 58(1): 184-189. |
| [5] | 高雅静, 李正芳, 马梦思, 武丽君. SII和SIRI对白塞病葡萄膜炎的风险预测及疾病活动度和预后的评估[J]. 北京大学学报(医学版), 2025, 57(6): 1067-1073. |
| [6] | 郭博达, 陆敏, 王国良, 张洪宪, 刘磊, 侯小飞, 赵磊, 田晓军, 张树栋. 肾透明细胞癌与非透明细胞癌伴静脉癌栓患者的临床病理特征及预后比较[J]. 北京大学学报(医学版), 2025, 57(4): 644-649. |
| [7] | 李伟浩, 李晶, 张学民, 李伟, 李清乐, 张小明. 术中回收式自体输血对颈动脉体瘤切除术后肿瘤预后的影响[J]. 北京大学学报(医学版), 2025, 57(2): 272-276. |
| [8] | 刘苗雨, 王思源, 裴林, 王殊. 同步应用戈舍瑞林对年轻乳腺癌患者新辅助化疗疗效的影响[J]. 北京大学学报(医学版), 2025, 57(2): 291-297. |
| [9] | 毛雅晴, 陈震, 于尧, 章文博, 刘洋, 彭歆. 2型糖尿病对口腔鳞状细胞癌患者预后的影响[J]. 北京大学学报(医学版), 2024, 56(6): 1089-1096. |
| [10] | 罗丹, 黄海建, 陈新, 陈小岩. 原发子宫肝样腺癌2例临床病理分析及文献复习[J]. 北京大学学报(医学版), 2024, 56(6): 1126-1131. |
| [11] | 欧俊永,倪坤明,马潞林,王国良,颜野,杨斌,李庚午,宋昊东,陆敏,叶剑飞,张树栋. 肌层浸润性膀胱癌合并中高危前列腺癌患者的预后因素[J]. 北京大学学报(医学版), 2024, 56(4): 582-588. |
| [12] | 刘帅,刘磊,刘茁,张帆,马潞林,田晓军,侯小飞,王国良,赵磊,张树栋. 伴静脉癌栓的肾上腺皮质癌的临床治疗及预后[J]. 北京大学学报(医学版), 2024, 56(4): 624-630. |
| [13] | 虞乐,邓绍晖,张帆,颜野,叶剑飞,张树栋. 具有低度恶性潜能的多房囊性肾肿瘤的临床病理特征及预后[J]. 北京大学学报(医学版), 2024, 56(4): 661-666. |
| [14] | 周泽臻,邓绍晖,颜野,张帆,郝一昌,葛力源,张洪宪,王国良,张树栋. 非转移性T3a肾细胞癌患者3年肿瘤特异性生存期预测[J]. 北京大学学报(医学版), 2024, 56(4): 673-679. |
| [15] | 方杨毅,李强,黄志高,陆敏,洪锴,张树栋. 睾丸鞘膜高分化乳头状间皮肿瘤1例[J]. 北京大学学报(医学版), 2024, 56(4): 741-744. |
|
||
