北京大学学报(医学版) ›› 2025, Vol. 57 ›› Issue (4): 692-697. doi: 10.19723/j.issn.1671-167X.2025.04.010
基于锥形束CT的前列腺癌放射治疗两种体位固定方式摆位误差比较
刘杰, 马茗微*( ), 王庆安, 石明, 尹金鹏, 王占平, 申静涛, 高献书
), 王庆安, 石明, 尹金鹏, 王占平, 申静涛, 高献书
- 北京大学第一医院放射治疗科, 北京 100034
Comparison of setup errors between two immobilization methods in prostate cancer radiotherapy based on cone-beam computed tomography
Jie LIU, Mingwei MA*(), Qing'an WANG, Ming SHI, Jinpeng YIN, Zhanping WANG, Jingtao SHEN, Xianshu GAO
- Department of Radiation Oncology, Peking University First Hospital, Beijing 100034, China
摘要:
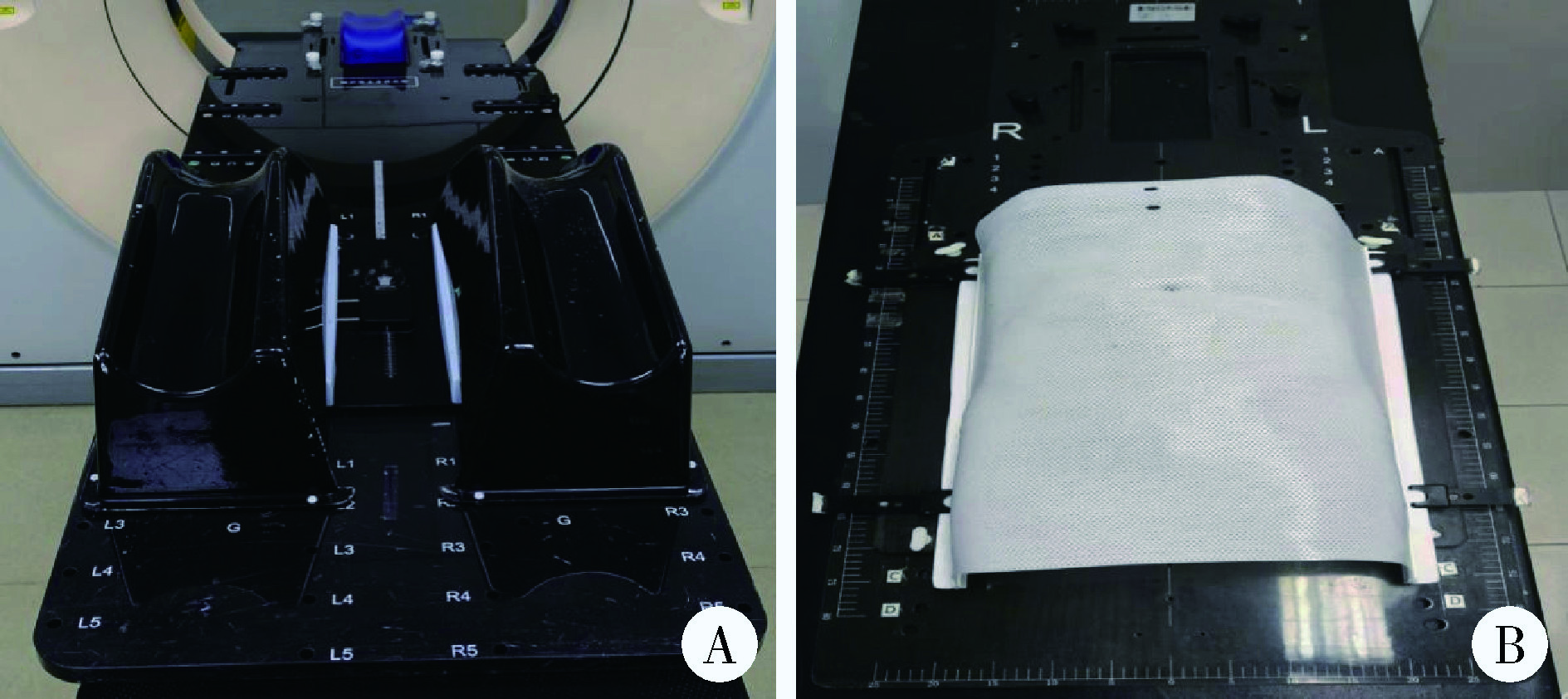
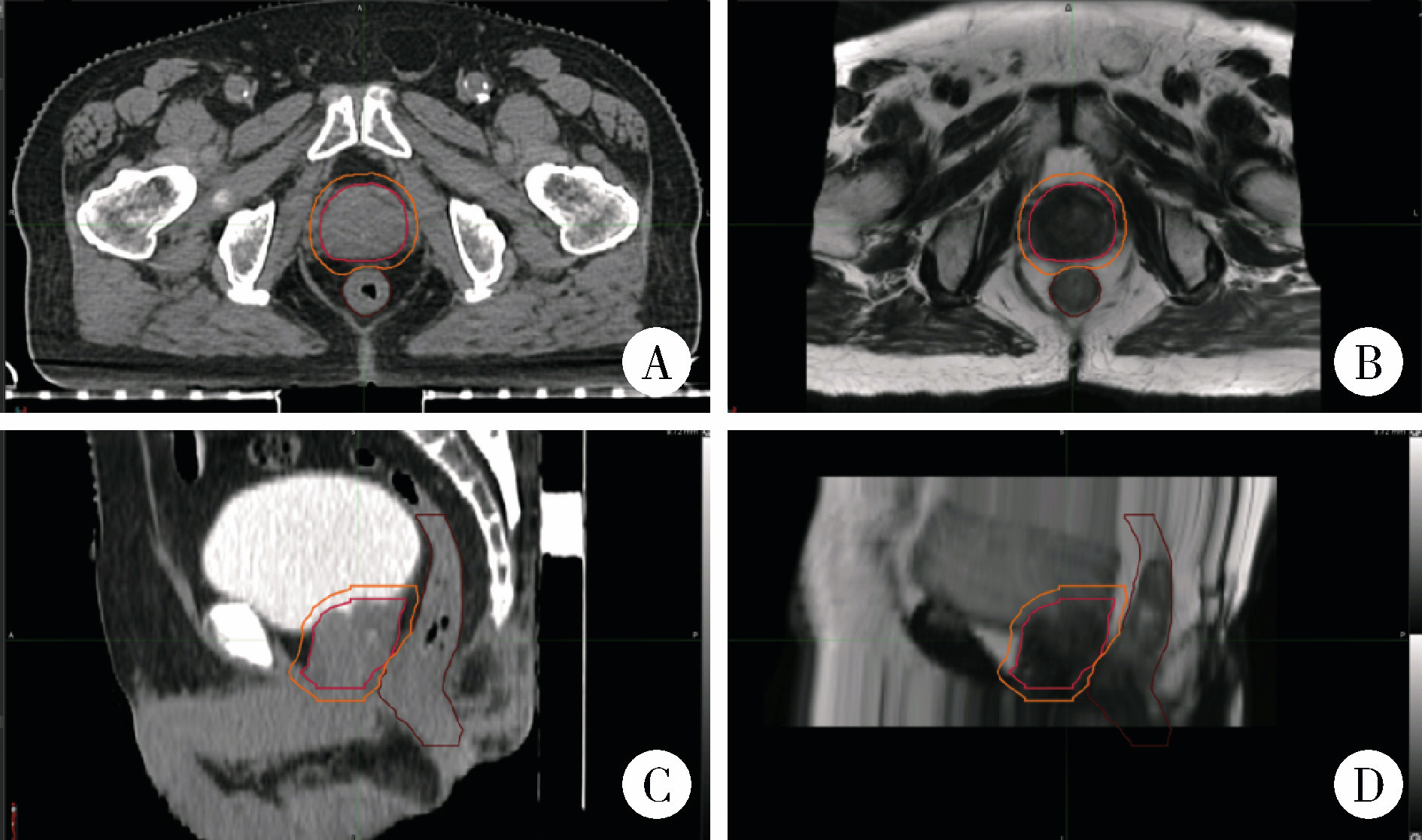
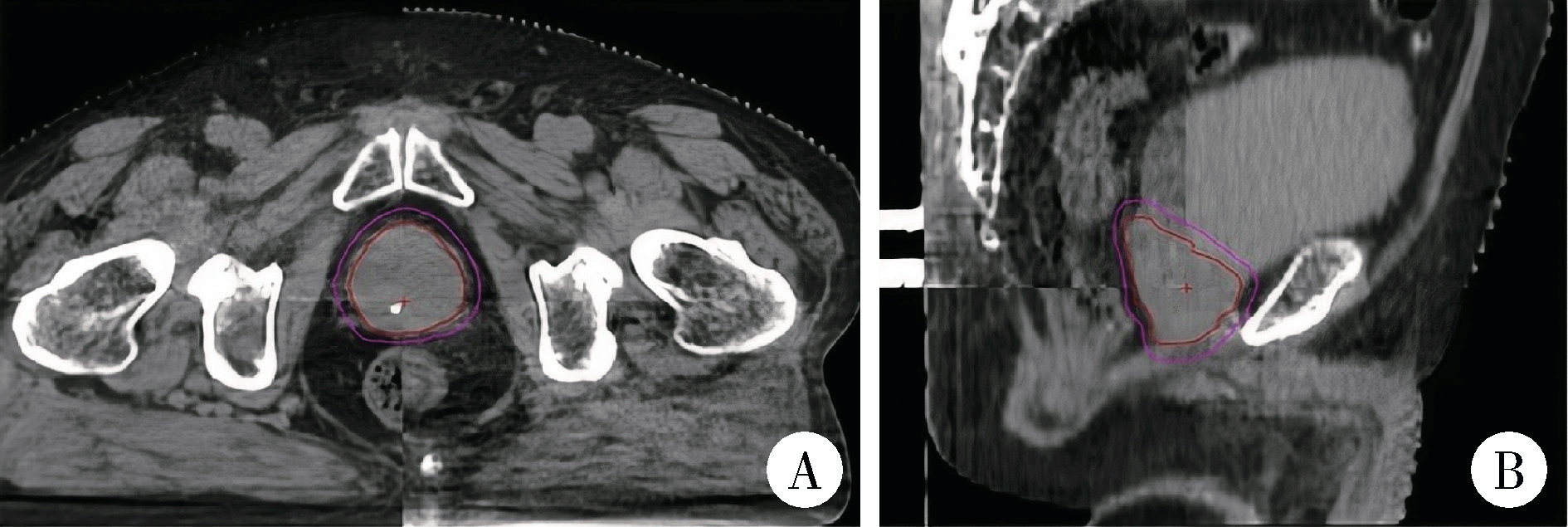
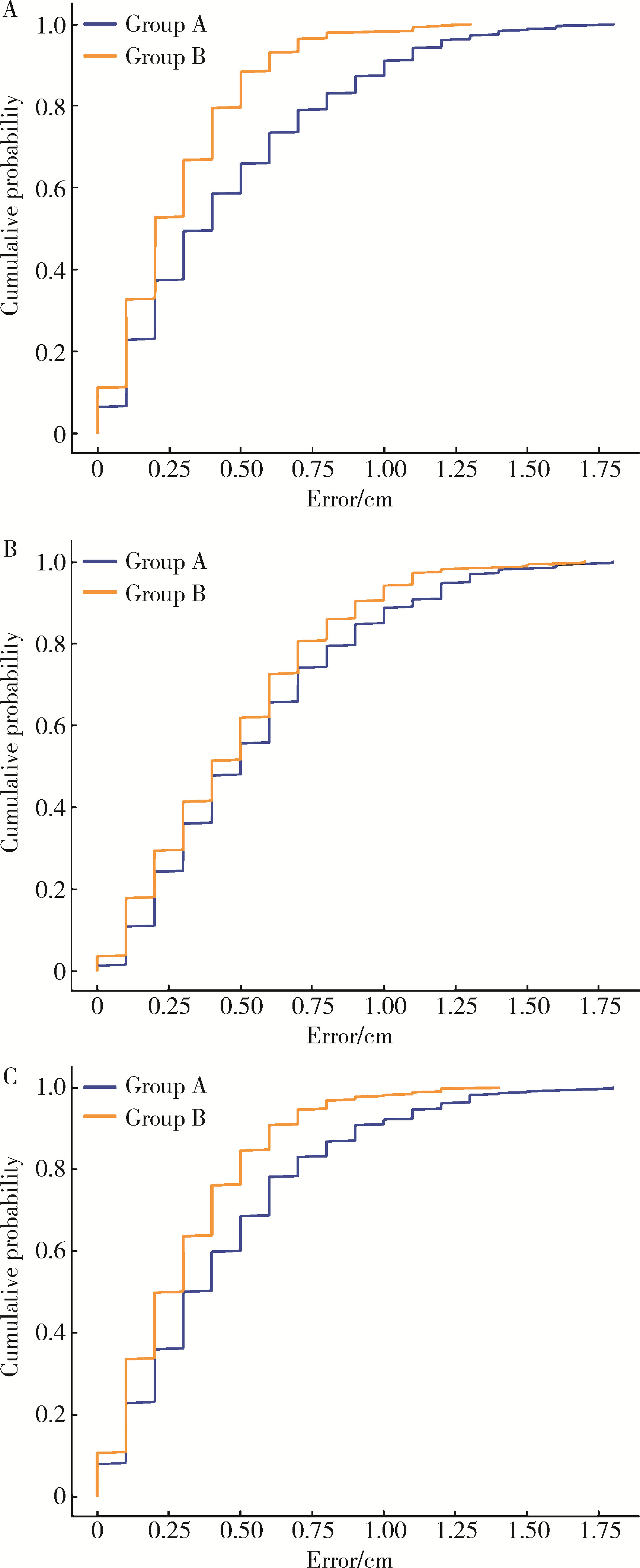
目的: 分析并比较前列腺癌根治性放射治疗中两种体位固定方式(截石位碳纤维全身固定架与常规碳纤维人体固定架结合热塑膜)的分次间摆位误差, 并计算两种方式下的临床靶区(clinical target volume, CTV)-计划靶区(planning target volume, PTV)外扩距离(margin for planning target volume, MPTV), 以优化体位固定方式和放射治疗流程。方法: 连续性纳入2021年8月至2023年3月在北京大学第一医院接受前列腺癌根治性放射治疗的37例患者的病例资料进行回顾性分析, 按体位固定方式分为两组[A组采用截石位碳纤维全身固定架18例, 共450组锥形束CT(cone-beam computed tomography, CBCT)图像, B组采用常规碳纤维人体固定架结合热塑膜19例, 共461组CBCT图像]。所有患者均行每日锥形束CT图像引导, 采用骨配准结合手动配准方法获取左右(X轴)、头脚(Y轴)及前后(Z轴)方向上的摆位误差数据。采用独立样本t检验和Mann-Whitney U检验和卡方检验比较两组摆位误差, 计算平均摆位误差、系统摆位误差(Σ)和随机摆位误差(δ), 并利用公式MPTV=2.5Σ+0.7δ计算CTV-PTV外扩距离。结果: 两组患者在三维方向上的摆位误差差异均有统计学意义(P均 < 0.01), A组X、Y、Z轴方向误差绝对值的M (P25, P75)分别为0.40(0.20, 0.70) cm、0.50(0.30, 0.80) cm和0.35(0.20, 0.60) cm, 而B组相应数值显著降低至0.20(0.10, 0.40) cm、0.40(0.20, 0.70) cm和0.20(0.10, 0.40) cm。Mann-Whitney U检验结果显示各方向差异具有统计学意义(X轴: z=-6.86;Y轴: z=-2.76;Z轴: z=-5.71)。在摆位误差位移量≤0.5 cm的累积分布中, A组和B组的比例分别为X轴297(66.0%)和408(88.5%)(P0.01)、Y轴250(55.6%)和285(61.8%)(P=0.055)、Z轴308(68.4%)和391(84.8%)(P < 0.01)。两组的CTV-PTV外扩距离分别为X轴0.66 cm和0.35 cm, Y轴0.67 cm和0.45 cm, Z轴0.54 cm和0.42 cm。结论: 常规碳纤维人体固定架结合热塑膜能显著减少摆位误差。在X、Y、Z轴三个方向上, 截石位碳纤维全身固定架的摆位误差较常规碳纤维人体固定架结合热塑膜更大, 因此需要进一步优化其摆位流程。由于截石位碳纤维全身固定架固定方法是经会阴超声引导技术中不可或缺的体位固定方式, 未来需针对其进行深入研究和改进, 以实现更高的摆位精度。
中图分类号:
- R737.25
| 1 |
|
| 2 |
|
| 3 |
|
| 4 |
|
| 5 |
|
| 6 |
|
| 7 |
|
| 8 |
|
| 9 |
|
| 10 |
马广栋, 洪莉. 宫颈癌的图像引导放疗研究综述[J]. 中国医疗设备, 2018, 33(5): 117-120, 129.
|
| 11 |
于松茂, 孟繁里, 康加阜, 等. 真空垫制作方式对肺癌立体定向放疗摆位精度影响研究[J]. 医疗卫生装备, 2019, 40(12): 33-35, 40.
|
| 12 |
马茗微, 王淑莲, 覃仕瑞, 等. 面罩及乳腺托架固定下乳腺癌保乳术后放疗锁骨上下区摆位误差分析[J]. 中华放射肿瘤学杂志, 2019, 28(3): 217- 221.
|
| 13 |
|
| 14 |
高研, 高献书, 马茗微, 等. 前列腺癌放疗时CBCT使用频率和匹配策略的剂量学分析[J]. 中华放射肿瘤学杂志, 2024, 33(8): 733- 739.
|
| 15 |
|
| [1] | 王月, 梁宇红. 繁茂型牙骨质-骨结构不良1例[J]. 北京大学学报(医学版), 2026, 58(1): 220-224. |
| [2] | 杨小勇, 张帆, 马潞林, 刘承. 前列腺导管腺癌临床特征及腺外侵犯的影响因素[J]. 北京大学学报(医学版), 2025, 57(5): 956-960. |
| [3] | 田素青, 孙海涛, 赵田地, 王巍. 6D治疗床辅助影像引导下放射治疗头颈部肿瘤摆位误差分析[J]. 北京大学学报(医学版), 2024, 56(6): 1097-1100. |
| [4] | 黄教悌,胡菁,韩博. 治疗相关神经内分泌前列腺癌机制研究与靶向治疗新进展[J]. 北京大学学报(医学版), 2024, 56(4): 557-561. |
| [5] | 邢念增,王明帅,杨飞亚,尹路,韩苏军. 前列腺免活检创新理念的临床实践及其应用前景[J]. 北京大学学报(医学版), 2024, 56(4): 565-566. |
| [6] | 颜野,李小龙,夏海缀,朱学华,张羽婷,张帆,刘可,刘承,马潞林. 前列腺癌根治术后远期膀胱过度活动症的危险因素[J]. 北京大学学报(医学版), 2024, 56(4): 589-593. |
| [7] | 于书慧,韩佳凝,钟丽君,陈聪语,肖云翔,黄燕波,杨洋,车新艳. 术前盆底肌电生理参数对前列腺癌根治性切除术后早期尿失禁的预测价值[J]. 北京大学学报(医学版), 2024, 56(4): 594-599. |
| [8] | 薄士仕,高承志. 基于卷积神经网络实现锥形束CT牙齿分割及牙位标定[J]. 北京大学学报(医学版), 2024, 56(4): 735-740. |
| [9] | 章锦花,潘洁,孙志鹏,王霄. 不同根管内容物对口腔颌面锥形束CT诊断牙根纵裂准确性的影响[J]. 北京大学学报(医学版), 2023, 55(2): 333-338. |
| [10] | 叶佳学,梁宇红. 牙髓专科医师应用锥形束CT的现况调查[J]. 北京大学学报(医学版), 2023, 55(1): 114-119. |
| [11] | 潘孟乔,刘建,徐莉,徐筱,侯建霞,李小彤,王晓霞. 牙周-正畸-正颌联合治疗骨性安氏Ⅲ类错 |
| [12] | 高娟,吕航苗,马慧敏,赵一姣,李小彤. 锥形束CT三维体积测量评估骨性Ⅲ类错 |
| [13] | 刘圣杰,侯惠民,吕政通,丁鑫,王璐,张磊,刘明. 双极雄激素序贯免疫检查点抑制剂治疗转移性去势抵抗性前列腺癌4例[J]. 北京大学学报(医学版), 2022, 54(4): 766-769. |
| [14] | 刘伟涛,王怡然,王雪东,周彦恒. 锥形束CT研究上颌反复扩缩前方牵引后上颌骨缝的三维变化[J]. 北京大学学报(医学版), 2022, 54(2): 346-355. |
| [15] | 白杲琛,宋毅,金杰,虞巍,何志嵩. 多西他赛联合卡铂治疗转移性去势抵抗性前列腺癌的临床疗效[J]. 北京大学学报(医学版), 2021, 53(4): 686-691. |
|
||
