北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (4): 684-687. doi: 10.19723/j.issn.1671-167X.2020.04.016
尿流率视觉量表的开发
张维宇,王焕瑞,刘献辉,王涛,陈京文,孙屹然,张晓鹏,胡浩,许克新( )
)
- 北京大学人民医院泌尿外科,北京 100044
Primary development of visual uroflow scale
Wei-yu ZHANG,Huan-rui WANG,Xian-hui LIU,Tao WANG,Jing-wen CHEN,Yi-ran SUN,Xiao-peng ZHANG,Hao HU,Ke-xin XU()
- Department of Urology, Peking University People’s Hospital, Beijing, 100044, China
摘要:
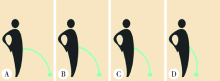
目的: 开发尿流率视觉量表(visual uroflow scale, VUS),分析量表评分与自由尿流率检查指标的相关性,应用VUS评估排尿功能,提高临床工作效率。方法: 招募2016年3月至2017年3月因下尿路症状(lower urinary tract symptoms, LUTS)就诊于北京大学人民医院泌尿外科的男性患者,进行自由尿流率检测前,患者先进行尿流率视觉量表评分。通过自由尿流率检测,获取最大尿流率、平均尿流率、排尿量等数据信息,并分析其与VUS的相关性。收集124例患者信息,其中53例符合纳入标准。采用Spearman相关性分析对VUS和自由尿流率变量以及患者年龄进行分析。结果: 大多数患者能在第一时间选择最符合自己的图,通过Spearman相关性分析发现,排尿时间与VUS呈正相关(相关系数0.62, P<0.05)。选择第3、第4幅图的患者往往排尿时间更长,提示更严重的LUTS。尿流时间与VUS呈正相关(相关系数0.61,P<0.05),当患者选择更高的VUS分数时,意味着不管尿等待时间多长,这部分患者会花更长的时间来排尿。最大尿流率和平均尿流率均与VUS呈负相关(相关系数为-0.54和-0.62,P<0.05), 提示VUS可以较准确地反映最大尿流率和平均尿流率水平。VUS与年龄呈正相关,反映排尿功能随年龄增长下降。结论: VUS能帮助临床医生初步判断患者排尿功能,患者在接受手术或药物治疗前先进行VUS评估,治疗后再进行评估,所得的量化数据可用于评估治疗效果。考虑到VUS方便、省时、易懂, VUS可能非常适合用于随访。
中图分类号:
- R69



| [1] |
Martin SA, Haren MT, Marshall VR, et al. Members of the florey adelaide male ageing study. Prevalence and factors associated with uncomplicated storage and voiding lower urinary tract symptoms in community-dwelling Australian men[J]. World J Urol, 2011,29(2):179-184.
doi: 10.1007/s00345-010-0605-8 pmid: 20963421 |
| [2] |
Kupelian V, Wei JT, O’Leary MP, et al. Prevalence of lower urinary tract symptoms and effect on quality of life in a racially and ethnically diverse random sample: the Boston area community health (BACH) survey[J]. Arch Intern Med, 2006,166(21):2381-2387.
pmid: 17130393 |
| [3] |
Madersbacher S, Alivizatos G, Nordling J, et al. EAU 2004 guidelines on assessment, therapy and follow-up of men with lower urinary tract symptoms suggestive of benign prostatic obstruction (BPH guidelines)[J]. Eur Urol, 2004,46(5):547-554.
doi: 10.1016/j.eururo.2004.07.016 pmid: 15474261 |
| [4] |
Fusco F, Groutz A, Blaivas JG, et al. Videourodynamic studies in men with lower urinary tract symptoms: a comparison of community based versus referral urological practices[J]. J Urol, 2001,166(3):910-913.
pmid: 11490244 |
| [5] |
Zhang W, Zhang X, Li H, et al. Prevalence of lower urinary tract symptoms suggestive of benign prostatic hyperplasia (LUTS/BPH) in China: results from the China health and retirement longitudinal study[J]. BMJ Open, 2019,9(6):e022792.
pmid: 31221864 |
| [6] |
Drach GW, Layton TN, Binard WJ. Male peak urinary flow rate: relationships to volume voided and age[J]. J Urol, 1979,122(2):210-214.
doi: 10.1016/s0022-5347(17)56333-8 pmid: 459016 |
| [7] |
Jörgensen JB, Jensen KM, Bille-Brahe NE, et al. Uroflowmetry in asymptomatic elderly males[J]. Br J Urol, 1986,58(4):390-395.
doi: 10.1111/j.1464-410x.1986.tb09092.x pmid: 3756408 |
| [8] | Siroky MB, Olsson CA, Krane RJ. The flow rate nomogram: Ⅱ. Clinical correlation[J]. J Urol, 1980,123(2):208-210. |
| [9] | Richmond SJ, Gunadasa S, Bland M, et al. Copper bracelets and magnetic wrist straps for rheumatoid arthritis-analgesic and anti-inflammatory effects: a randomised double-blind placebo controlled crossover trial[J]. PLoS One, 2013,8(9):e71529. |
| [10] | Ender SA, Wetterau E, Ender M, et al. Percutaneous stabilization system Osseofix® for treatment of osteoporotic vertebral compression fractures: clinical and radiological results after 12 months [J]. PLoS One, 2013,8(6):e65119. |
| [11] | Kersten P, White PJ, Tennant A. Is the pain visual analogue scale linear and responsive to change? An exploration using Rasch analysis[J]. PLoS One, 2014,9(6):e99485. |
| [12] | Lukacz ES, Lawrence JM, Burchette RJ, et al. The use of visual analog scale in urogynecologic research: a psychometric evaluation[J]. Am J Obstet Gynecol, 2004,191(1):165-170. |
| [13] |
Selekman RE, Harris CR, Filippou P, et al. Validation of a visual prostate symptom score in men with lower urinary tract symptoms in a health safety net hospital[J]. Urology, 2015,86(2):354-358.
pmid: 26169006 |
| [14] |
Memon MA, Ather MH. Relationship between visual prostate score (VPSS) and maximum flow rate (Qmax) in men with urinary tract symptoms[J]. Int Braz J Urol, 2016,42(2):321-326.
doi: 10.1590/S1677-5538.IBJU.2015.0032 pmid: 27256186 |
| [15] |
van der Walt CL, Heyns CF, Groeneveld AE, et al. Prospective comparison of a new visual prostate symptom score versus the international prostate symptom score in men with lower urinary tract symptoms[J]. Urology, 2011,78(1):17-20.
doi: 10.1016/j.urology.2011.01.065 pmid: 21550646 |
| [1] | 冷汶远, 高端, 李晓宇, 左炜, 胡伟民, 朱振鹏, 徐纯如, 林健, 李学松. 口腔黏膜补片与脱细胞真皮基质补片治疗长段尿道狭窄的疗效和安全性对比[J]. 北京大学学报(医学版), 2025, 57(5): 975-979. |
| [2] | 牛远杰, 辛钟成, 林桂亭, 丁攀, 潘建成, 封玉宏, 郭应禄. 低强度激光疗法治疗男性生殖与性功能障碍[J]. 北京大学学报(医学版), 2025, 57(4): 627-632. |
| [3] | 李宗瀚, 黄洋阅, 李宁, 李明磊, 宋宏程, 张潍平, 刘超. 国产单孔蛇形臂机器人手术系统在儿童肾盂成形术中的应用[J]. 北京大学学报(医学版), 2025, 57(4): 662-665. |
| [4] | 张启鸣, 陈泽波, 田雨, 潘大猛, 刘磊, 张洪宪, 赵磊, 张树栋, 马潞林, 侯小飞. 机器人辅助腹腔镜移植肾切除术经验总结[J]. 北京大学学报(医学版), 2025, 57(4): 666-669. |
| [5] | 余霄腾, 黄奕瑄, 李新飞, 陈昶甫, 赵方舟, 应鸿刚, 陶子豪, 张一鸣, 徐丽清, 李志华, 杨昆霖, 周利群, 李学松, 赵峥. 结石相关输尿管狭窄的上尿路修复手术技术与临床结局[J]. 北京大学学报(医学版), 2025, 57(4): 670-675. |
| [6] | 冀竞辉, 林秀石, 潘大猛, 吴芝莹, 薛子璇, 田晓军, 张树栋, 王滨帅, 邱敏. 输尿管硬镜联合勺状阻石篮激光碎石术治疗输尿管1.5 cm及以上结石的效果[J]. 北京大学学报(医学版), 2025, 57(4): 676-683. |
| [7] | 左超, 王国立, 杨昆霖, 车新艳, 孟一森, 张凯. 前列腺体积不同的患者经尿道光纤铥激光前列腺剜除术的有效性及安全性比较[J]. 北京大学学报(医学版), 2025, 57(4): 711-716. |
| [8] | 王起, 柯涵炜, 丁泽华, 张维宇, 张晓鹏, 徐涛, 许克新. 耻骨后与经闭孔尿道中段悬吊术对术后最大尿流率及残余尿量的影响[J]. 北京大学学报(医学版), 2025, 57(4): 717-720. |
| [9] | 陈千喜, 陈延, 郑仲杰, 唐文豪, 刘镇, 洪锴, 林浩成. 辅助生殖技术周期中不同睾丸取精方式下非梗阻性无精子症患者的精子库供精比例[J]. 北京大学学报(医学版), 2025, 57(4): 721-726. |
| [10] | 刘世豪, 徐丽清, 李新飞, 杨昆霖, 李兆莹, 张子博, 王祥, 傅炜骁, 李志华, 李学松. 国产模块化手术机器人系统辅助肾盂成形术的可行性和安全性评价[J]. 北京大学学报(医学版), 2025, 57(4): 779-783. |
| [11] | 王焕瑞, 赖世聪, 胡浩浦, 丁泽华, 徐涛, 胡浩. 腹腔镜与输尿管软镜联合定位治疗复杂输尿管狭窄的疗效分析[J]. 北京大学学报(医学版), 2025, 57(4): 784-788. |
| [12] | 黄万伟, 沙显燊, 张艺宝, 伍国豪, 骆峰, 陈智慧, 叶东明, 李学松, 赖彩永. 完全3D腹腔镜回肠代双侧输尿管联合膀胱扩大术修复放射治疗后双侧输尿管狭窄并膀胱挛缩[J]. 北京大学学报(医学版), 2025, 57(4): 789-795. |
| [13] | 徐啸, 王海东, 刘振华, 夏海缀. 气肿性肾盂肾炎:单中心经验总结[J]. 北京大学学报(医学版), 2025, 57(4): 812-816. |
| [14] | 姜瑞, 兰孝达, 张喆楠, 肖云翔, 吴士良, 何志嵩, 李学松, 韩文科, 张骞, 孟一森. 动脉输尿管瘘3例[J]. 北京大学学报(医学版), 2025, 57(2): 408-410. |
| [15] | 刘宁, 满立波, 何峰, 黄广林, 翟建坡. 良性前列腺增生患者排尿中断症状与尿动力学指标的相关性[J]. 北京大学学报(医学版), 2025, 57(2): 328-333. |
|
||
